











































Communications, Immunization, and Polio Vaccines: Lessons from a Global Perspective on Generating Political Will, Informing Decision-Making and Planning, and Engaging Local Support
World Health Organization, or WHO (Menning, Rosenbauer); Gavi, the Vaccine Alliance (Garg); Eastern and Southern Africa Regional Office, United Nations Children's Fund, or UNICEF (Pokharel); Pan American Health Organization, or PAHO (Thrush); Programme Division, UNICEF (Farrell, Malik); Task Force for Global Health (Veira, Wanyoike, Patel); Western and Central Africa Regional Office, UNICEF (Kodio)
"Central to the success of the communications function in driving this program was its ability to generate a meaningful policy dialogue about polio vaccines and routine immunization. This dialogue was vital to fostering stakeholder participation and ownership, strengthening partner coordination, guiding implementation, and facilitating an iterative process of feedback and learning."
This paper, included in a special open-access edition of The Journal of Infectious Diseases exploring polio endgame activities, reports on the strategic planning processes, technical approaches, and lessons learned by the Communications Working Group (CWG), which may be relevant to other global health initiatives with similarly complex mandates and accelerated timelines. In particular, it examines the group's driving of all of the communications-related activities related to the implementation of inactivated poliomyelitis vaccine (IPV) introduction and the switch from trivalent OPV, or tOPV (containing types 1, 2, and 3 poliovirus) to bivalent OPV, or bOPV (containing types 1 and 3 poliovirus). This switch, which was carried out as part of objective 2 of the Polio Eradication and Endgame Strategic Plan 2013-2018, "called for intense global communications and coordination on an unprecedented scale from 2014 to 2016, involving global public health technical agencies and donors, vaccine manufacturers, World Health Organization and United Nations Children's Fund regional offices, and national governments....While the success of the milestones achieved proves that such a globally coordinated initiative is feasible, the lessons raise a number of important considerations for the role of global-level communications in building awareness and commitment, informing national decision-making and planning, and building local-level support and acceptance."
Pending certification of the eradication of type 2 poliovirus, a tentative timeline of April 2016 was scheduled (and confirmed in October 2015) for the globally synchronised switch from trivalent OPV (containing types 1, 2, and 3 poliovirus) to bivalent OPV (containing types 1 and 3 poliovirus) in all 155 OPV-using countries and territories. The importance of communications to objective 2 of the Endgame Plan was evident from the start. At the outset, the new Global Polio Eradication Initiative (GPEI) programme requirements were perceived as challenging to communicate, difficult to understand, unrealistic in terms of timelines, and potentially infeasible for logistical implementation.
In that context, the CWG, co-chaired by the WHO and UNICEF, brought together a diverse set of skills in global and national communications and advocacy, representing public health partners and academic institutions (e.g., the WHO, UNICEF; Emory University; the Centers for Disease Control and Prevention; Gavi, the Vaccine Alliance; the Task Force for Global Health; Rotary International; and the Bill and Melinda Gates Foundation). As the work of the CWG advanced over time, a standardised method was established for the planning, development, and dissemination of guidance and materials, together with regular forums for input and dialogue. This familiar mode of operation for all work (concerning IPV introduction and the OPV switch) offered the benefits of active participation of all key stakeholders and helped to build wide ownership for and uptake of the group’s outputs.
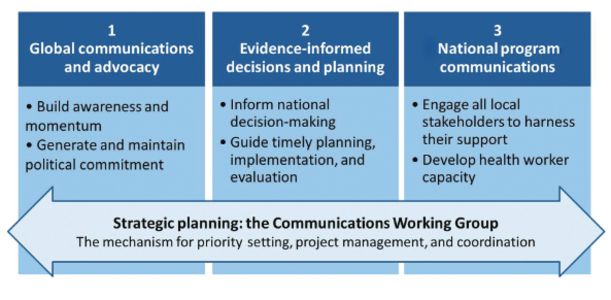
The CWC established a number of core areas of work for communications:
Generating awareness and political commitment via global communications and advocacy - At the beginning of preparations for both IPV introduction and the OPV switch, a detailed communications plan was generated by the CWG and reviewed by the Immunization Systems Management Group (IMG), which had set up the CWG. This plan outlining the core objectives, risks and opportunities, audiences, messaging, materials, timelines, and responsibilities was found to be particularly critical for harmonising activities with the milestones of technical implementation and for anticipating and overcoming any possible challenges. It also ensured that all key stakeholders were actively engaged in a manner corresponding to their role and function, gaining their buy-in via early involvement in the planning process.
The entire process and approach is described, including the activities around the OPV switch in 155 countries and territories in a 2-week period in April 2106. The CWG started early in 2015 and proceeded methodically, developing a comprehensive plan and then a package of initial materials, including a high-level briefing note, an introductory PowerPoint presentation to introduce the technical rationale and early considerations for national planning, and a frequently asked questions document. Given the potential risk of misrepresenting the global withdrawal of trivalent OPV, all messaging was carefully crafted and recognised as crucial to forming a common global vocabulary and understanding. A press release and media briefing was conducted in mid-April 2016, accompanied by donor and partner briefings. "Analyses of global media coverage, representing >70 articles on the OPV switch, showed that global media featured accurate and accessible explanations of the switch, in part because of the longstanding relationships with many key health journalists. Additionally, reporting from regional and country-based partners affirmed the wide uptake and use of all CWG materials and templates."
Lessons learned:
- Build strong awareness among global partners and national decision-makers through regular dialogue and links to accessible and relevant information. Establish an up-to-date, intuitively designed website as a core reference for all materials in multiple languages.
- Situate IPV introduction and the OPV switch in the larger context of polio eradication and opportunities for routine immunisation strengthening.
- Develop trusting relationships and facilitate an enabling environment with global and regional colleagues and partners by facilitating open dialogue in orientations, briefings, or workshops, combined with a 2-way exchange of information and inputs.
- Equip and empower advocates and influential stakeholders with adaptable tools and resources, to encourage ownership and leadership.
- Package messaging and materials based on levels of complexity, targeted per audience, in modular and adaptable formats, and in multiple languages for easy local adaptation.
Informing national decision-making, planning, and implementation - While the initial phases of work were dedicated to raising awareness and informing decision-making, the accelerated timelines required that efforts rapidly move to focus on planning and preparations for implementing IPV and the OPV switch. The CWG was responsible for coordinating the development of guidance and various adaptable tools and templates (e.g., for budgeting, logistics, communications, and monitoring and validation) - all designed to simplify and accelerate the national planning processes, and to offer sound programmatic recommendations as a basis for local implementation. Recognising the importance of a systematic and transparent decision-making process to eventual community acceptance of the new vaccine, discussions on outstanding topics helped to engage local leaders and stakeholders. To assist, a comprehensive information kit targeted to National Immunization Technical Advisory Groups, or their equivalent, was developed and disseminated, encompassing the WHO policy recommendations, evidence base, operational guidance, and supporting materials. Case studies and short documentary-style videos on the introduction of IPV in early adopter low- and middle-income countries were also seen to be particularly useful for sharing learning and best practices. One approach that proved to be particularly effective in generating momentum for IPV introduction was the organisation of region-specific workshops and consultant trainings in late 2014, followed by full-day sessions during regional immunisation manager meetings in early 2015.
Lessons learned:
- Disseminate a complete and modular package of evidence and materials specifically designed for national immunisation technical advisory groups, immunisation programme managers, policymakers at various levels, and ministries, to support informed decision-making.
- Ensure that information and communications about the rationale are sufficient to reach all relevant personnel in countries, in appropriate detail and complexity per intended audience.
- Map a plan for the phased release Of communications materials and operational guidance (especially when in unchartered territory), starting with the broader principles and high-level steps before expanding on the details.
- Maintain an ongoing 2-way dialogue With all regions, colleagues, and partners, inviting feedback from all to inform planning and refinement Of materials and messages, particularly in relation to complex subject matter.
- Mobilise and accelerate national-level planning and preparations through the availability of technical guidance, supported by a range of user-friendly and adaptable tools. These materials should be anticipated and developed well in advance, for timely dissemination.
Conducting in-country programme communications and capacity building to ensure acceptance of IPV and continued uptake of OPV - Similar questions were being asked all around the world: Why should our infants receive 2 vaccines, IPV and OPV, against the same disease? How are these vaccines different? Are 3 injections during a single visit risk free? Is OPV still safe and effective? Answers would eventually be locally adapted and context-specific, ideally based on the findings of formative research or surveys. To accelerate the implementation of local communications activities, the CWG disseminated a variety of globally developed guidance materials and adaptable templates on IPV and the OPV switch in multiple languages. This helped to maintain a consistent and accurate message, and it expedited national efforts to produce and finalise content. In-country activities also worked to ensure that local experts, medical associations, civil society, traditional leaders, and journalists would become partners and contributors to a positive communications environment. Specific to the OPV switch, there were complexities of the rationale and potential for misinterpretation of the vaccine safety–related reasons for withdrawal of trivalent OPV. Thus, at a global level, the general recommendation to countries was to avoid any proactive public communications but, instead, to focus on targeted engagement of well-informed and key stakeholders to contribute to an accurate local dialogue. One vital activity was the training of health workers and other immunisation personnel to build the skills and knowledge needed to correctly handle and administer the polio vaccines and capably explain the programme changes to caregivers and local communities.
Lessons learned:
- Develop an evidence-informed and budgeted national communications plan at least 3 months in advance, including an outline of intended audiences, approaches, key messages, and activities. Where resources allow, the plan should be informed by the findings of formative research or similar assessments of knowledge, attitudes, and behaviours.
- Leverage messaging and communications activities to establish a link to immunisation and disease eradication goals and to reinforce the importance of timely vaccination.
- Mitigate communications risks by conducting workshops, briefings, or trainings with influential stakeholders and reporters, to share information in advance, and facilitate a 2-way dialogue to understand and respond to concerns and generate buy-in.
- Mobilise religious and community leaders, schoolteachers, and students to support the introduction of the new vaccine and assist in tracking defaulters.
- Ensure that a crisis communications plan in place, with a prepared statement, messaging, and procedures, to enhance readiness and response times in the case of any event.
- Advocate for and mobilise sufficient resources for the development and implementation of communications plans at all levels.
The report examines the CWG's strategic planning, describing, for instance, how the format of the work plan, at times covering >50 different activities, was established as a collective tool and brought transparency and accountability to the responsibilities and timelines. Fortnightly teleconferences were among the manifestations of the group's emphasis on participatory dialogue, which helped to ensure its effectiveness in engaging all partners, seeking and acting on inputs, and in producing quality outputs. Other factors contributing to the CWG's success are: leadership; expertise; ability to adapt or innovate; responsiveness to needs; mutual accountability; and continuity of participants. Lessons learned:
- Establish a strong team with diverse communications skill sets, representing the core partner organisations at a global and regional level. This team will serve a number of functions, including (i) contributing to the development of materials and providing expert input when called upon and (ii) drawing on its network to support the dissemination of materials and related gathering of inputs.
- Create mechanisms for regular communications and dialogue among team members - electronic, via phone, and in person - for information sharing, for troubleshooting, and for encouraging constructive and open discussion.
- Ensure that feedback loops and channels for input are well functioning, to build ownership and trust, to benefit future new and updated materials and approaches, and to capture and draw on practical lessons from countries in respective regions.
- Adopt best practices for project management and tracking of activities, priorities, timelines, and responsibilities, ideally in a manner that offers transparency and mutual accountability.
- Plan ahead, anticipating potential challenges and barriers and allowing sufficient time for consultations and testing of materials before timely dissemination.
In concluding, it is noted that, in addition to reaching its programmatic goals, the ripple effect on reinforcing technical capacity at all levels should be noted, even if only an indirect outcome of the CWG. Beyond 2016, the level of intensity of the CWG will decrease, but a new communications plan has been developed to help manage information and expectations in the post-tOPV era, during which will exist the risk of vaccine-derived poliovirus outbreaks, continued IPV shortage, and remaining needs to document and promote the lessons learned. "These efforts will contribute to securing the gains made by countries in stopping polio transmission and preparing for full OPV cessation, as the world moves into the final stages of eradication."
Three case studies are provided at the end of the report to offer a more in-depth review of specific topic areas where tailored communications strategies were a key factor to their success.
The Journal of Infectious Diseases, Volume 216, Supplement 1: S24-S32. DOI: https://doi.org/10.1093/infdis/jix059.
- Log in to post comments