











































Finding the Signal through the Noise: A Landscape and Framework to Enhance the Effective Use of Digital Social Listening for Immunisation Demand Generation
HealthEnabled
"For those working to manage the infodemic, filtering the overabundance of information and public response can be challenging. How do teams decide what is important to respond to, what rumour is gaining traction and what is best left alone? For health and communications teams with limited capacity, where is effort best placed for maximum public health impact?"
The so-called infodemic accompanying the COVID-19 pandemic has seen misinformation and disinformation - including around vaccines - spread quickly, especially on social media. Listening to people's perspectives on and concerns about immunisation expressed online and in other forms of communication can inform strategies to tackle vaccine hesitancy and encourage more people to get vaccinated. Social listening data collection tools range from artificial intelligence (AI) and machine learning platforms to telephone hotlines, broadcast radio talk shows, and documentation of community dialogues. This report provides an overview of digital approaches to social listening for immunisation and proposes a framework with practical guidance for those seeking to use this approach to strengthen vaccine demand. The work was led by Health Enabled with technical guidance and support from a global partnership consisting of the World Health Organization (WHO), Gavi, The Vaccine Alliance, the United Nations Children's Fund (UNICEF), and the Vaccination Demand Hub.
WHO has been working with partners since March 2020 to develop tools and systems to help countries effectively manage the overabundance of information associated with the pandemic. Recommendations from the 4th Virtual WHO Infodemic Management Conference: Advances in Social Listening for Public Health (see video, below) highlighted the need to increase accountability, triangulate data, work from an evidence base, and improve global coordination. The WHO public health research agenda calls for more clarity and guidance on social listening, and the analysis offered in this report seeks to answer that call.
The landscape analysis involved a combination of desk research, key informant interviews, a review of relevant frameworks, and evidence/learning from country experiences. The report offers four case studies provide examples of different country experiences - Indonesia, Pakistan, South Africa, and Burkina Faso - in harnessing aspects of social listening data and analysis to engage effective actions to improve vaccine acceptance.
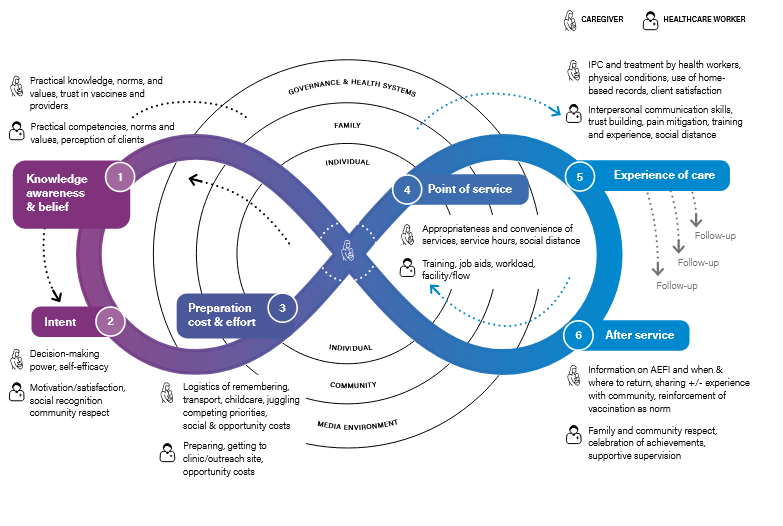
The report builds on models used to understand vaccine demand, such as UNICEF's Journey to Health and Immunisation (see figure above), the Vaccine Misinformation Management Field Guide (see Related Summaries, below), and other behavioural science frameworks that explore the social and contextual determinants of vaccine acceptance. These frameworks highlight the need for immunisation programmes to focus on key drivers of demand, including:
- Trust in people, institutions, and what contributes to local determinants of trust;
- Sources of community influence;
- The vaccine decision-making process, including social and contextual influences;
- Community access to services; and
- Quality of care, interpersonal communication, and client perceptions of the services.
The task of translating public conversations about vaccination into effective action for public health is complex, so the report offers a process map identifying stages, including:
- Analyse the context and situation, asking: What are the main bottlenecks to vaccine demand? Hoaxes and disinformation? Misinformation and hesitancy? Supply challenges? Trust and transparent communication? Access to correct and current information? Customer satisfaction?
- Identify existing data sources, asking: What sources of data already exist to inform the state of vaccine demand? What additional sources could be added with current capacity and resources? Examples include community feedback, routine immunisation data, digital media monitoring, and knowledge, attitude, and practice (KAP) surveys.
- Identify trusted influencers, sources of information, and partners (e.g., with civil society organisations (CSOs), non-governmental organisations (NGOs), health worker associations, and local community influencers and leadership in order to: create buy-in for the process and priorities, establish roles and responsibilities, share data and input on barriers to vaccination, and develop a coordinated and strategic response to needs and gaps identified through social listening.
- Understand-analyse, asking: What approaches can find actionable insights from the existing data? How much time and resources are available for data analysis and interpretation? This step may involve data aggregation and visualisation, qualitative analysis, and automated approaches.
- Engage: Based on findings from data collection and analysis, implement locally tailored and targeted approaches that address programme priorities and identified demand bottlenecks.
- Measure and monitor impact: Learn from experiences by measuring changes in public conversations and sentiment; include plans to address identified capacity and resource gaps; and use lessons and results to advocate to national health and Expanded Programme on Immunisation (EPI) community on the importance and utility of vaccine demand data.
Specific recommendations are included for different levels of involvement in social listening. Here are selected examples for:
- Programme implementers - e.g.:
- Triangulate multiple data sources: No single source of social listening data can provide a complete picture of current opinions, barriers, and challenges.
- Build platforms for inter-agency coordination on social listening, as these processes should not happen in silos. Risk communication and community engagement (RCCE) approaches need to be harmonised and complementary.
- Consider the goal of social listening activities and the existing data ecosystem to create an optimal mix of sources that will address priority vaccine demand bottlenecks. Map the context-specific trusted sources of information and communication, media types, social media, and digital penetration in different groups.
- Create a library of tested content, messages, and communication channels to rapidly respond to critical situations detected in social listening activities.
- Policymakers - e.g.:
- Dedicate capacity and resources to develop strategic and evidence-based risk communication teams as part of the national immunisation programme.
- Support a foundation of digital and health literacy in the general population to foster long-term resiliency and resistance to misinformation and disinformation.
- Ensure that appropriate policies and legal environment exists to safeguard data privacy and security at all stages of social listening activities.
- Be aware of the objectives of different agencies and enterprises providing services or platforms for social listening. Be clear with any providers on how they are managing data privacy, security, and data ownership.
- Researchers - e.g.,
- Identify and share priority learning questions that can be answered through implementation research by country teams that are building systems and learning from experiences.
- Develop methods and approaches for understanding and measuring how different categories of demand data (e.g., social media monitoring, KAP surveys, sentinel community surveillance) accurately represent the sentiments and perceptions of the local community. How does exposure to misinformation via different sources impact vaccine hesitancy and other health behaviours?
- Research the theory of change of social listening: What are the steps between identifying someone retweeting a vaccine-sceptical message and someone else choosing whether to be immunised?
- Ensure that experiences, evaluations, and lessons learned from social listening for vaccine hesitancy are transparent, documented, and shared.
- Funders - e.g.:
- Invest in national capacity, tools and resources for robust immunisation communications teams for data management, analysis, and risk communications.
- Encourage and support the development of tools and approaches that can be tailored to country needs and can provide data and analyses at sub-national levels.
- Consider including funding for social listening, digital demand generation, and infodemiology management as a core component of budgets for immunisation programmes.
- Support the development and sharing of experiences on methods and best practices for selecting, implementing and evaluating effective vaccine demand communication messages.
The researchers caution that, while new digital tools used commercially for social listening in high-income countries could add great value to vaccine demand generation in low- and middle-income countries (LMICs), further evidence is needed before providing sound, evidence-based guidance for resource-constrained countries. It is as yet unproven whether these applications lead to improved actionable information that justify the cost, both in money and in the limited capacity of small communications teams in LMICs.
In conclusion: "Social media insight is only useful if it leads directly to communications and other interventions to improve demand for vaccination. Social listening is not an end in itself - it must be embedded in the wider health system, to be a channel for communications so that the system can respond to the concerns of the population. The response to community insights should not just be 'messaging' to communities. When concerns are raised,...health system officials need to take time to reflect on the insights, consider adaptations of ways of working and then share how the health system will respond to the concerns raised by communities (closing the feedback loop). Trust can only be built by providing evidence that the health system is listening and that there is a willingness to work in partnership with communities."
WHO website, August 18 2021 - accessed on October 26 2021. Image credit: from Human-Centred Approach for Health
- Log in to post comments