











































Home-Based Record Redesigns That Worked: Lessons from Madagascar & Ethiopia
This document from JSI's Coordination and Implementation of Child Health Record Redesigns Project summarises two home-based records (HBR) redesign efforts in Madagascar and Ethiopia, including the background and rationale for considering a redesign, the stakeholders involved, and the steps completed in the process to redesign and roll out a revised HBR (sometimes called immunisation cards or child health booklets). Challenges and lessons learned from both countries are also explored. Building on these experiences, similar cards have been designed and used in Ghana, Liberia, Myanmar, and elsewhere; the Madagascar and Ethiopia case studies can inform countries who may be interested in undertaking their own redesigns.
HBRs are described here as a data collection and monitoring tool serving multiple purposes for the caregiver, health worker, and health system. These records can: (a) aid health workers in documenting and tracking which vaccines have been given to a child; (b) empower a parent or caregiver to play a role in the health of their children; and (c) serve as public health monitoring tools on vaccination coverage through household and other surveys. However, research has shown that HBRs have often been under-utilised in immunisation programmes. Historically, many countries have used a traditional format that may not be easy for health workers to complete accurately or for caregivers to understand. Also, various users may not understand the value of these documents. Redesign approaches in some countries have been successful in meeting the needs of health workers, caregivers, and the health system, while also increasing the availability and use of HBRs (with an overall objective of increasing immunisation coverage).
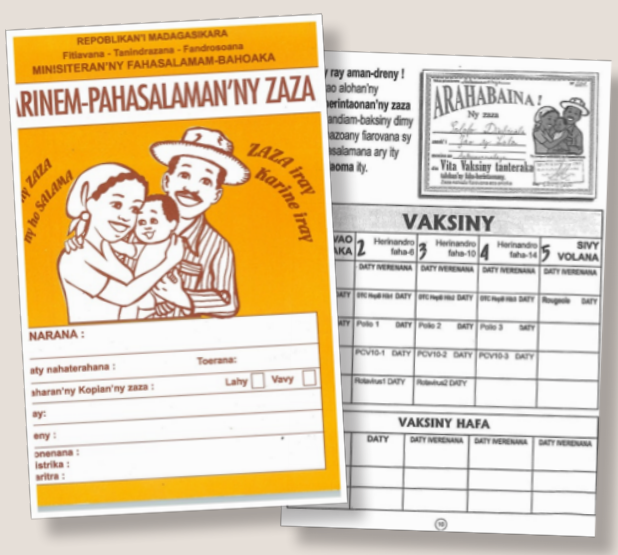
Madagascar's experience shows that a user-centred approach was integral to the development of the new HBR. The process, which began in 1997 and is described in detail in the report, featured the Ministry of Health (MOH) creating an Information, Education and Communication (IEC) Taskforce to provide oversight of communications materials, including the HBR. A local designer was contracted in the initial HBR resdesign through the Basic Support for Institutionalizing Child Survival (BASICS) project; he has continued to develop health communications materials for many projects and the MOH, thus adding to the consistency and recognition of the illustrations in the HBR and other health materials. Early HBR designs were shared with health workers and communities through focus group discussions conducted with community representatives and caregivers to solicit feedback. These inputs were then discussed with the IEC Taskforce and the designer, with revisions then made based on this feedback. At least two different versions of a design were tested. Village meetings were held to: (1) encourage community involvement, (2) orient them on the health indicators and messages/actions included in the HBR, and (3) increase the value placed on maternal and child health programmes, including the HBR. Volunteer Community Agents served as mobilisers and reinforced the use of these tools. A promotional campaign was developed, which included intense marketing to families. Messaging was developed to show that the new HBR was modern and empowering: as a tool for families to know their child's health status and as a document that parents themselves could review and own (i.e., the content was not just for the health workers or mobilisers). Rapid project assessments showed that once 20% or more of families started using the HBR, it began to catch on - as the "model families" introduced the importance of the HBR to others. The experience from Madagascar showed that families and communities could be engaged through small do-able actions that were included in the HBR for caregiver and health worker reference and use.
Similar to Madagascar, the involvement of end-users was an integral part of the HBR development in Ethiopia. The same designer who developed the Madagascar HBR was sent to Ethiopia to support their original redesign, and he worked with a local, Ethiopian designer who subsequently completed later revisions/updates. In Ethiopia, the new HBR included detailed pictures and child survival and nutrition messages, which were meant to make it easy for health workers and promoters to draw the interest of mothers - particularly those who were non-literate. This HBR was supported by the LINKAGES project and later by the Integrated Family Health Program (IFHP). However, the new card was never able to supplant the traditional World Health Organization (WHO) immunisation card because of reasons such as lack of advocates at the higher level to make a change to the HBR from the older card. Without support at the regional level, including training and practical application, health extension workers may not recognise the importance of this new tool.
In short, although the pathways were similar in Madagascar and Ethiopia, JSI's informational interviews showed that the long-term sustainability and use of the "new" HBRs differed greatly: Madagascar has continued to use the redesigned HBR with minor tweaks and additions, while Ethiopia uses a similar version of the redesigned HBR, but as a communication tool for health promoters (i.e., not as a filled-in vaccination record for each child), with the redesigned version never completely replacing the older, WHO vaccination card for data entry. Both countries introduced the redesigned HBR as part of an intervention package and larger communication strategy. Thus, the impact of solely the redesigned HBR is difficult to measure, but project findings showed increased coverage correlated with the new HBR. (See pages 8-9 of the report for data.)
Considerations from these HBR redesign experiences are related to:
- Stakeholder engagement - Actively include the following in redesign: end-users (health workers, parents and caregivers, and the health system); Expanded Programme on Immunization (EPI) and other programmes (e.g., maternal, newborn, and child health, or MNCH) with sections in the HBR; the United Nations Children's Fund (UNICEF), WHO, and other partners (e.g., the United States Agency for International Development (USAID) and other bilaterals or donors); Ministry of Finance; and a graphic designer.
- Redesign - Consider these elements:
- Find a competent, professional designer.
- Use a simple design and format.
- Minimise illustrations to those that are meaningful to users.
- Include only key information that can be recorded and monitored for action.
- Test HBR with various user groups before finalising.
- Importance of cards as part of a communications strategy - Although the card was originally designed as a record of immunisations (and other health services) received by a child, the role of the HBR has now expanded to serve other purposes, such as a behaviour change communication tool. In both Madagascar and Ethiopia, the new HBR was introduced as part of a larger intervention that included a diploma that families received once their child is fully immunised. A study in Ethiopia in June 2006 found that, among those who publically received the printed diploma, behaviours were more likely to be sustained 6-12 months later.
- Card sustainability - Part of the introduction process is upfront planning and securing financing for printing and distribution longer-term. Without these resources in place, no matter how well designed the new HBR is, it will not succeed.
"The most important lesson that was shared by all is that just redesigning an HBR is not enough to ensure increased availability and use. Many other factors go into the successful redesign and roll-out, including: (1) ensuring that cards are printed in sufficient, long-term supply, (2) making arrangements for distribution to districts, then to health facilities, and finally to health promoters and caregivers; (3) conducting training on why the cards are important tools; and (4) supporting follow-up review meetings and formative supervision to emphasize the use of cards. This requires a sustained commitment from the MOH to ensure success and often the support from other partners. It is also important to limit and simplify the messages that are included, as families can be overwhelmed by the number of health actions they are to take, and health promoters need guidance on how to use the HBR. The most successful HBRs have a balance between behavior change messages and as a reporting tool for services received."
"Specific findings related to design elements included ensuring that the HBR is easy for parents to navigate and understand which can include color coding each section and the use of graphics and acceptable images/pictures. The design should also be simple for health promoters and health workers to reference and complete. Lastly, when designing a new card or redesigning with additional content, it is important to build-in opportunities and financing for monitoring and evaluation in order to track availability and use. This should be a shared responsibility by all MOH programs that have content in the HBR."
TechNet-21 and JSI website - both accessed on November 17 2017; and email from Kirstin Krudwig to The Communication Initiative on November 28 2017.
- Log in to post comments