











































Placing Human Behavior at the Center of the Fight to Eradicate Polio: Lessons Learned and Their Application to Other Life-Saving Interventions
United Nations International Children's Emergency Fund, or UNICEF (Guirguis, Obregon, Coleman, Hickler); Harvard T. H. Chan School of Public Health (SteelFisher)
"For the field of public health, the lesson to place human factors - how people think, make choices, and behave - at the center of disease control initiatives is a lesson that the world cannot afford to overlook again."
This report, included in a special open-access edition of The Journal of Infectious Diseases exploring polio endgame activities, articulates what happened when the Global Polio Eradication Initiative (GPEI) began to pay more attention to the dynamics of human and social behaviour change. "As the initiative accumulated success and setbacks, it became evident that the success of eradication depends not only on technical innovation or organizational and political commitment, but also on successfully engaging communities for prolonged periods. In parallel, the setbacks the global eradication program has faced in different settings have all too often arisen because individual and community engagement were inadequate or not prioritized."
The analysis draws on key reports and documents of polio eradication efforts (e.g., peer-reviewed literature and reports by the GPEI and the GPEI Independent Monitoring Board), with a particular focus on social, behavioural, and communication dynamics. The article is heavily informed by the authors' long-time engagement with policy, evidence and research, and implementation aspects of the global polio eradication efforts.
Three particular lessons for other health and immunisation programmes can be drawn from the experience of GPEI and are elaborated here. In brief:
- Behaviour change must come first from individuals and organisations themselves before change can be seen in the communities with whom we seek to engage. This lesson is exemplified by the experience of the GPEI in India, beginning in the early 2000s. The paper describes the work of the Social Mobilization Network (SMNet), a network of women built by UNICEF in 2001 in Uttar Pradesh to serve as a bridge between the polio programme and the communities it served by facilitating dialogue and trust in communities with the largest burden of poliovirus. Mothers from the community were trained as community mobilisation coordinators and tasked with speaking to other mothers about children's health, the importance of taking the polio vaccine repeatedly, and quelling concerns about its safety. The India experience demonstrated several new lessons for the GPEI: (i) community demand and support could either facilitate or erode progress toward eradication, (ii) women engaging with other women is a successful strategy to build trust and facilitate access to more children, and (iii) innovations need time and space to fail and adapt, to benefit from local knowledge, and to be monitored to see whether they can breed success. Despite the lessons from India and the literature supporting female-to-female peer engagement, employment of women to build trust with other mothers for polio in the most conservative areas was only starting to be accepted by many governments and development officials in the GPEI by 2015. Perhaps one explanation for the fact that it took the GPEI almost 2 decades to recognise the importance of human and social factors in disease control and a decade to fully implement a proven and effective strategy to build trust in just 3 polio-endemic countries can be found in the World Bank's 2015 World Development Report, which posited that "development professionals, like everyone else, are themselves subject to the biases and mistakes that can arise from thinking automatically, thinking socially, and using mental models."
- Good data are not enough for good decision-making. Through a partnership launched in 2013 between UNICEF and the Harvard Opinion Research Program at the Harvard T. H. Chan School of Public Health, an initiative was developed to produce credible social data that could be used to inform global policy and behaviour change strategies across polio-affected countries. A conceptual framework was created to measure 4 dimensions of trust: competence, morality, compassion, and concern for the child. Though the examples of data that emerged from what are described here as high-quality knowledge, attitudes, and practices (KAP) studies based on in-depth understanding of the audiences' concepts, the paper points out that a set of standardised, credible, and regularly collected data "has been of enormous benefit to the polio program: it has shifted behavioral strategies at global and country levels (see lesson 3), improved the integration of behavioral and social considerations into the operations of the program, and demonstrated the value that communications and social mobilization could have to reach more children with OPV [oral polio vaccine]." All that said: "Social data have been used only when there have been individuals and organizations with the skills and commitment to raise its significance to a level on par with that of epidemiological data and to mobilize stakeholders to act upon it. It has been more likely to be ignored when the evidence goes against popular, long-held beliefs of program practitioners or leaders or when it points to risks that the epidemiological data have not yet identified. Where it could be dismissed or misinterpreted by those that have a vested interest in the status quo, it has been too easy to do so."
- Health workers are important agents of behaviour change. As is noted here, where social data have been used, they have led to critical shifts in how the polio programme communicates and engages with communities. For instance, polling data demonstrated that there was a challenge of health worker trust in and negative social norms about polio vaccination among segments of the population that were most critical for eradication. These data led to a new global communications strategy that focused on: (i) promoting all vaccination as a social norm, (ii) creating mass media campaigns that were more emotionally resonant and less exclusively driven by information and awareness, (iii) building trust and goodwill for health workers by humanising them, and (iv) building a new brand for the polio programme that could reinforce positive reforms recently implemented. The strategy was first rolled out in Pakistan in 2015. Vaccinators were exposed to a new, integrated approach that incorporated interpersonal communications throughout the full vaccinator training curriculum. Social insights were also integrated into the recruitment of health workers to ensure that they had a profile that each community felt would build trust. Once the recruitment and training strategy of health workers began to be realised in the field, a mass media campaign was overhauled with a new brand that promoted health workers as sehat muhafiz ("protectors of health") and showed them as integral parts of the community (mothers, fathers, and daughters themselves), gender appropriate, ethnically relevant (>90% of cases occurring in 2013 and 2014 were among Pashtuns), and demonstrating genuine concern for children while vaccinating them. Thanks to such an approach, Pakistan has 56% fewer polio cases in 2016 than it did at the same time in 2015. In a 2016 poll, 72% of caregivers in the districts at highest risk for polio said their experience with vaccinators was "better" than their experience with those who visited their homes a year earlier (i.e., before the strategy was rolled out).
These reflections and articulations of lessons learned lead to some conclusions and recommendations, such as:
- "Health and immunization programs seeking to invest in a more effective and sustainable model should prioritize behavioral and social factors from the inception of program design."
- "Programs seeking to invest in a more robust evidence base for vaccine demand or outbreak response should not only build systems that can collect rigorous, reliable social data but must simultaneously invest in health systems and organizational cultures that are held accountable for implementing health programs that incorporate epidemiological and social data."
- "To succeed, this new model must remove the financial and reputational disincentives to learn from failure; they must be equipped to make timely adjustments if data come back demonstrating that an intervention or assumption requires modification."
- "To truly place human factors at the forefront of health and immunization programs, we must be willing to listen to what the people we are trying to serve actually want, even when this defies our own expertise and our individual experience."
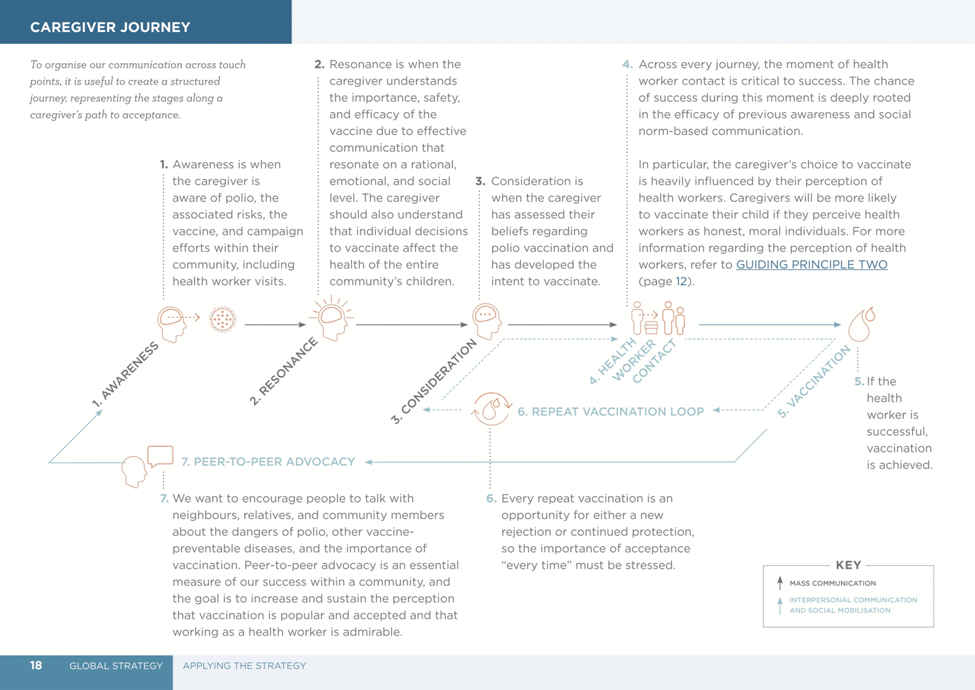
The Journal of Infectious Diseases, Volume 216, Supplement 1: S331-S336. DOI: https://doi.org/10.1093/infdis/jiw546. Image caption/credit: "The caregiver journey to OPV acceptance. The figure originally appeared in the Polio Communication Global Guide."
- Log in to post comments