











































Transmission of Vaccination Attitudes and Uptake Based on Social Contagion Theory: A Scoping Review
University of Cyprus (Konstantinou, Georgiou, Kyprianidou, Nicolaides, Karekla, Kassianos); Yale University (Kumar); MIT Sloan School of Management (Nicolaides); University College London (Kassianos)
"Public health authorities should tailor interventions and involve family and friends to result in greater vaccination uptake."
Vaccine hesitancy is a complex health problem, with various factors involved, including the influence of an individual's social network. According to the Social Contagion Theory (SCT), an individual can exhibit behaviour modelled by another person or adopt the attitudes of members of their social network. Based on the belief that SCT can inform public health policies and interventions to improve vaccination rates, this scoping review aims to collate evidence on how attitudes and vaccination uptake are spread within social networks. It was conducted at the height of the COVID-19 pandemic in 2020, when vaccines were produced and distributed. Thus, rapid evidence was needed in order to inform policies on tackling vaccination hesitancy and to provide guidance on rolling out national vaccination campaigns effectively.
Databases of PubMed, PsycINFO, Embase, and Scopus were searched, and 11 cross-sectional studies, published between 2011 and 2020, were included in the final analysis. Most of the included studies used social network analysis to examine influence of social networks on vaccination attitudes and uptake (n = 7, 63.6%), with the remaining studies using logistic regression models. All studies used egocentric networks (networks of individuals that are mapped with information provided on their ties) to examine the outcomes of vaccination attitudes and uptake.
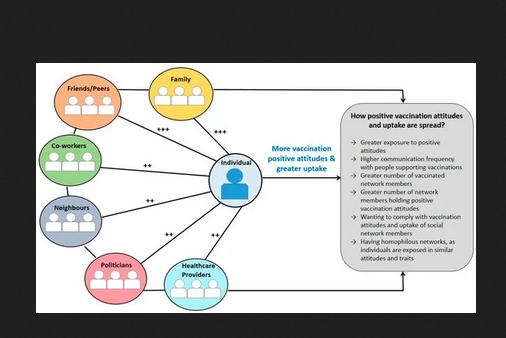
Across studies, vaccination attitudes and uptake of participants were highly influenced by their social networks (see Figure 2 in the paper, and above, for a summary). Positive attitudes on self and childhood vaccinations (e.g., that vaccines are safe and effective) were influenced by social networks' positive attitudes, whereas having vaccinated people in networks was related to increased likelihood of participants to be vaccinated or vaccinate their child. Similarly, negative attitudes (e.g., beliefs that vaccines are dangerous or unsafe) and lower vaccination uptake were influenced by social networks' negative attitudes and lower uptake.
Most of the included studies (n = 8, 72.7%) reported that family and friends/peers significantly influenced self and childhood vaccination attitudes and uptake. In contrast, only two studies reported that healthcare providers and co-workers - and one study that politicians - significantly influenced vaccination attitudes and uptake. Some studies found that participants held more positive attitudes towards self and childhood vaccinations when they were discussing them with family and friends/peers who held similar attitudes, or when they perceived their family and friends/peers holding positive attitudes towards self and childhood vaccinations.
Accordingly, vaccination uptake for self or children increased when the individuals' network was comprised mostly by vaccinated family and friends or when parents observed their peers vaccinating their child. Conversely, vaccination uptake for self or children decreased if family and friends were vaccine hesitant or held negative attitudes toward vaccinations.
Regarding mechanisms underlying transmission within networks, frequency of communication between network members and prolonged exposure to positive or negative self and childhood vaccination attitudes explained transmission in social networks. However, the researchers stress that simply being exposed to or discussing vaccinations with others does not imply that an individual will adopt the same behaviour. Social transmission is a complex process involving an individual's knowledge, skills, motivation, attitudes, and opportunities provided by their network. For example, according to the COM-B model, a behaviour change may occur when an individual has opportunities to enable the behaviour such as positive support from family and friends together with other attributes such as the psychological and physical capacity, capabilities, and motivation to perform the behaviour. "Individuals may also adopt the vaccination attitudes of their social network or get vaccinated as a result of social norms; to fit in or to be socially accepted..."
Homophily - the tendency of similar individuals to be connected in a social network - was identified as a significant factor that drives the results, especially with respect to race and ethnicity. Therefore, individuals tend to have homogeneous networks (see Figure 2 in the paper, and above, for a summary of the mechanisms). These findings imply that targeting each network using tailored recommendations for campaign messaging, such as the use of short, risk-reducing, or relative risk framing messages with clear and simple language, could possibly reduce vaccine hesitancy.
Suggestions for further research based on the type of network (e.g., family), vaccination (e.g., human papillomavirus vaccine, or HPV), and attitude (i.e., positive vs. negative) are presented in Table 3. For example: Examine whether clustering exists with specific members of a social network and how it influences vaccination attitudes and uptake of individuals. Relatedly, future studies could examine the factors underlying how family and friends/peers influence vaccination attitudes and uptake compared to other network members.
Thus, this review highlights the key role that social networks play in shaping attitudes and vaccination uptake. "Since all people are connected to other people, the effects of an intervention which is delivered to an individual might be indirectly diffused to their social network....Clinicians and policymakers could consider network structure of for example communities and general practice patients, in order to result in higher diffusion of interventions' effect....In addition, clinicians and policymakers are recommended to include social network members in interventions or provide educational family-based programs on vaccinations."
Vaccines 2021, 9(6), 607; https://doi.org/10.3390/vaccines9060607.
- Log in to post comments