











































Understanding Vaccine Acceptance and Demand - and Ways to Increase Them
World Health Organization (WHO) Regional Office for Europe (Habersaat, Jackson); Valid Research Limited (Jackson)
"Informed by the theoretically and evidence-informed insights gained from research with target groups and engagement of key stakeholders (e.g. using the COM-B model to structure findings), interventions can be designed, implemented and evaluated with the aim to increase vaccination uptake."
Health authorities are tasked not only with offering vaccination services but also with ensuring easy and convenient access, supporting and promoting vaccination, and ensuring equitable extension of vaccination services to all. The World Health Organization (WHO) and its partner organisations have developed tools to support Member States in addressing vaccine acceptance and demand (defined as ranging from passive acceptance to active demand). Their approach, outlined in this article, involves recognising that both individual and context determinants influence vaccination behaviours and using a theoretical model that considers all potential barriers to ensure that interventions are evidence-informed and tailored to the local context.
The article's authors, Katrine Bach Habersaat and Cath Jackson, note that parental concerns about vaccine safety, myths and misperceptions about vaccination, and distrust in health authorities are often highlighted in the public debate as key reasons for low vaccination uptake and vaccine-preventable disease (VPD) outbreaks. They affirm that insights from psychology are critical to understanding individual reasons behind vaccine hesitancy and are useful for designing effective messages and education. However, they challenge the assumption that immunisation uptake can be increased through effective information campaigns alone, as there are multiple other determinants of vaccination intentions and behaviours. For instance, social and cultural factors and norms, including those that relate to certain religious, educational, or philosophical views, can influence attitudes to vaccination.
With this in mind, Habersaat and Jackson explain that the approach to ensuring increased uptake must be comprehensive and consider determinants that relate not only to the individual but also to the context (such as social, cultural, institutional, and political factors). Thus, achieving high and equitable vaccination uptake in all population groups is not a quick fix; it requires long-term investment in multifaceted interventions, informed by research with the intended population(s). The WHO Regional Office for Europe has adapted the COM-B model (Capability, Opportunity, Motivation-Behaviour) for their Tailoring Immunization Programmes (TIP) approach (for some CI offerings on TIP, see Related Summaries, below).
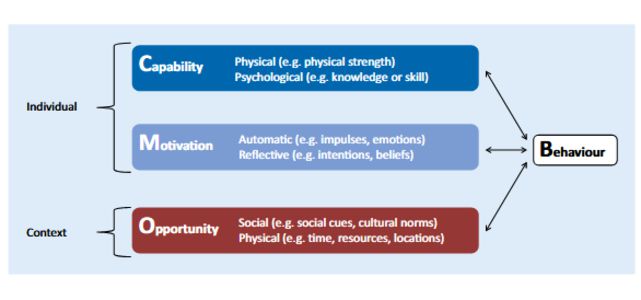
In short, the core of the COM-B model (see Figure 2, and above) features 3 factors (each of which has 2 sub-components) that need to be in place for any health behaviour to occur: capability, opportunity, and motivation. Capability and motivation factors are individual determinants, whereas opportunity factors are context determinants. The factors interact; capability and opportunity both influence motivation; and all 3 factors influence behaviour. Conversely, behaviour influences all 3 factors; in fact, past vaccination behaviours are predictors of future vaccination behaviours.
Some adaptation and simplification of the COM-B model has been made following testing of the model by national immunisation programmes in the Region. Experience to date has led to a vaccination adaptation of the COM-B model (see Figure 3) that considers: capability as one factor directed by both psychological and physical mechanisms; motivation as one factor directed by both reflective and automatic mechanisms; and opportunity as divided into 2 factors: physical and social. To illustrate the use of the adapted COM-B model, some examples of TIP projects from the WHO European Region, their intended populations, target COM factors, and interventions are presented in Table 2.
Habersaat and Jackson cite evidence showing that the encounter between the vaccine recipient/caregiver and the vaccination provider (doctor, nurse, health worker) is a critical moment in vaccination decision-making. Accordingly, they recommend that health authorities explore the barriers and drivers from the perspective of both groups of stakeholders. Infobox 1 in the paper shows an example of topics that can be explored for one factor (social opportunity) and 2 intended groups (caregivers and health workers).
They explain that, from the literature on vaccine hesitancy, acceptance, and demand, it is not possible to highlight just one strategy or a few specific interventions to increase vaccination uptake. However, some evidence exists on proven methods, such as, at the individual level, health workers providing face-to-face clear, balanced information about vaccination risks and benefits. However, there is a lack of large-scale implementation of these approaches to successfully show that people's vaccination perceptions can be changed. At the context level, there is more documentation for effective strategies, including those that focus on making vaccination the easy, convenient, and default behaviour and that focus on the interaction between caregivers and health workers.
Three recommendations emerge from the analysis, according to Habersaat and Jackson:
- Before any intervention is planned, gain insights into the drivers and barriers to vaccination in the key intended groups through empirical data and a situation analysis.
- Ensure that formative research and subsequent intervention development are informed by a theoretical model, such as the COM-B model or other health behaviour change models, as well as a planning framework, such as those available from WHO (e.g., TIP) and the United Nations Children's Fund (UNICEF) (e.g., the human-centred design (HCD) approach).
- Help address research gaps by pilot-testing, monitoring, and evaluating any approach to increasing vaccination uptake, wherever it is applied, and share both good and bad experiences.
Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2019 Dec 4. doi: 10.1007/s00103-019-03063-0.
- Log in to post comments