












































Advancing the Application of Systems Thinking in Health: Understanding the Growing Complexity Governing Immunization Services in Kerala, India
Public Health Foundation of India (Varghese); Sree Chitra Tirunal Institute for Medical Science and Technology (Kutty); Johns Hopkins University School of Public Health (Paina); World Health Organization (Adam)
"...the evidence base of public health programs, such as immunizations, should go beyond epidemiological and economic analysis. Our study emphasizes the need for public health governance systems to take into consideration the nature of multiple interactions when societies organize themselves to manage a public function like immunization."
This paper describes an application of systems thinking to understand the phenomena underlying changes in vaccination coverage in India. Specifically, it uses a complex adaptive system (CAS) lens to understand the features of a complex system that governs childhood immunisation in parts of the Indian state of Kerala, where immunisation coverage drastically declined after a period of high coverage in the late 1990s.
What happened with polio vaccination campaign in Kerala illustrates the nature of this rapid decline. In 1995, as part of the Global Polio Eradication Initiative (GPEI), additional oral polio vaccine (OPV) was administered to all children under 5 on 2 national immunisation days (NIDs). Despite initial opposition from some medical professionals, the campaign was generally well received, benefiting from ongoing civil society participation. The opposition was from some physicians in academic settings as well as some private doctors who questioned the need for additional OPV for a state like Kerala, when the state already had high routine immunisation coverage. Initial opposition was neutralised by the public's confidence in vaccination in general and considerable state support for the programme. In 2000, a case of polio was reported in Kerala. Although this event was seen as a failure of the public system, the impact on the immunisation programme was not immediately evident, and the efficacy or safety of the vaccine was not questioned. Yet this polio case was followed by a series of critical events related to immunisation-created feedback loops that influenced sudden changes to the social acceptability of vaccines. For instance, public protest carried out by the alternative medicine proponents against the Intensified Pulse Polio Immunisation (IPPI) campaign, which was launched in 1999, began to influence the community's trust in vaccines.
As explained here, in the context of the governance of public health interventions, such as immunisations, "complexity is generated from the diverse and dynamic nature of interactions between the system's actors and the multiple interacting factors such as values, culture, history, norms, and distribution of power and information in societies. Furthermore, the interconnectedness between the various actors of the system means that their actions inevitably create ripple effects that cause continuous change and adaptation of the intervention in the entire system." The idea is that exploring these complex system features in Kerala could shed light on the factors that drove unexpected changes in immunisation coverage and provide insights into the types of system adaptations that national immunisation programmes should consider.
A qualitative case study design was used to obtain an understanding of immunisation coverage in Kerala. Two districts in Kerala were randomly identified: Alappuzha, a better-performing (90.2%) district in terms of immunisation coverage as per the third District Level Health Service survey, and Kozhikode, a poorly performing (65%) district. The fieldwork included 7 participant and 7 non-participant multi-site observations, 5 focus group discussions, and 17 interviews with beneficiaries, community intermediaries (community health workers, nutrition and preschool teachers and community leaders), and providers from public and private sector. The study also involved key informant interviews with 6 experts. Furthermore, participant and non-participant observations were made with the help of an observation guide in order to gather insights into cultural meanings and interpretations related to provider and beneficiary behaviours and context. Participant observations were made during the house visits that the first author made along with community health workers, aiming to mobilising beneficiaries for vaccination. During each of the visits, the researcher was introduced to households as a public health researcher and was involved in motivating and educating the families on childhood vaccinations. Non-participant observations were made during immunisation sessions at health facilities, outreach immunisation sessions, and review meetings of field staff in charge of the immunisation programme.
The qualitative data showed a widespread hesitancy against routine vaccinations in Kozhikode district, while routine vaccinations are widely accepted in Alappuzha district. It was observed during the house visits in vaccine-resistant areas of Kozhikode district that most of the unvaccinated children are found in households of close geographical vicinities.
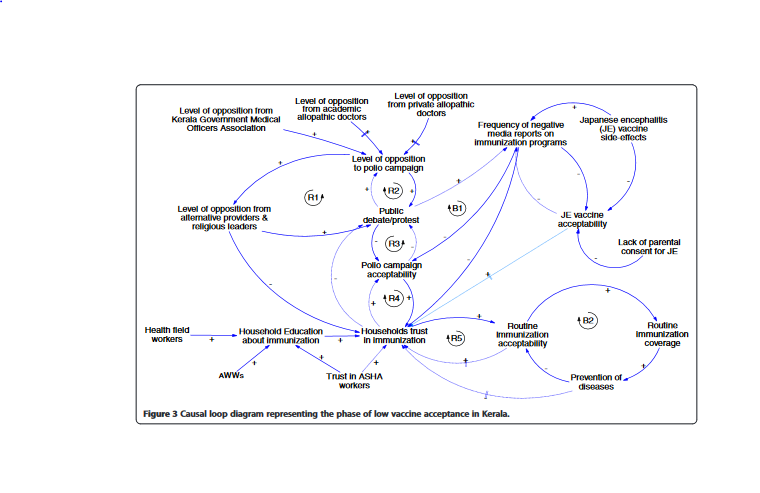
Content analysis was guided by features inherent to CAS such as phase transitions, feedback, path dependence, and self-organisation. Two causal loop diagrams (CLDs), such as the one above, were developed to depict the interactions among actors and critical events that contributed to phase transitions from vaccination acceptance to resistance. The researchers also describe the feedback that affected the districts differently after showing a high level of vaccine acceptability in the beginning. Next, they show how the authorities have responded to this problem of decline in immunisation coverage and discuss the impact of their response in the presence of certain highly connected actors playing a disproportionate influence over a household's vaccination decision. (For instance, "There was a greater likelihood that the male members [especially in northern Kerala] got influenced by external factors, such as the media and the public protests, used by the alternative medicines groups.")
Theoretical exposition of the findings reveals the important role of trust in health workers and institutions that shape the interactions of actors leading to CAS phenomena. For example, the findings reveal that from a period of suspicion and rejection, vaccines have achieved public confidence mainly through a positive feedback mechanism facilitated by its capacity to demonstrate reduction of diseases in the community. Information against immunisation programmes and the occasional reporting of vaccine-related adverse events following immunisation (AEFIs) undermined a household's trust in immunisations. In the context of a low burden of vaccine-preventable diseases (due to several years of good vaccination coverage), the reductions in trust created a negative feedback loop that dramatically affected vaccination acceptability and coverage. The researchers discuss the findings in the light of 2 theoretical interpretations of trust - trust in expert systems, and interpersonal trust - to understand the feedback and to explore strategies for the better governance of immunisation services.
The researchers suggest that the role that the media played in such contexts in informing households with conflicting messages on immunisation and how the key actors trusted each information requires attention. In Kerala, increased penetration of 24-hour local electronic news media and several widely read health publications are informing households on every AEFI and public debate on immunisation programmes. "Sensitizing the media for more responsible reporting and using it to convey appropriate health messages are options that public health departments may use in such situations, even though it is unlikely to eliminate all unwanted information from reaching households."
As illustrated in this study, a CAS lens can help researchers and decision makers to systematically explore the driving forces and factors in each setting and develop appropriate and timely strategies to address them. In the bureaucratic context of implementation of India's Universal Immunization Programme (UIP), there was limited recognition of the need to influence informal interactions in a way that retains trust in vaccines and in the public health department that governs immunisation programmes. The governance of immunisation was seen as an exercise to ensure control and order through top-down hierarchical interactions. The alternative perspective explored in this study, however, goes beyond the conventional assumption that the government's public health department is the sole governor of public health issues divorced from wider societal forces such as other key providers, social networks, and the households themselves with which the decision to vaccinate lie. The argument is that what is needed while formulating immunisation policies and programme strategies is careful consideration of multiple interactions involving the actors and their perceptions and ideas, which are shaped by factors such as trust.
Health Research Policy and Systems. 2014; 12: 47. doi: 10.1186/1478-4505-12-47
- Log in to post comments