












































Case Study: Innovations in Emergency Disease Responses
This study, which reports on a project conducted by the Centre for Research in Innovation Management (CENTRIM) at the University of Brighton that was funded by UKaid from the United Kingdom (UK)'s Department for International Development (DFID), seeks to analyse and explain how innovation works in emergency communicable disease responses. It does so through use of the concept of an innovation ecosystem, the set of factors and actors that come together in ways that might foster or inhibit effective innovation processes. It looks at innovations across the range of activities involved in communicable disease responses in emergencies, and seeks to better understand the ecosystem by reviewing both positive examples, where innovations have emerged and been successful (e.g., the response to polio outbreaks in Syria), and more challenging examples, where innovations have not happened, or where they have not been successful (e.g., Ebola in West Africa, and cholera in Haiti). The study reveals an innovation ecosystem that is good in certain parts, and at certain times, but which is heavily reliant on a number of critical internal actors and on external capacities and resources. Moreover, the ecosystem is far from systematic, and is not always well suited to the nature and dynamics of emergency work.
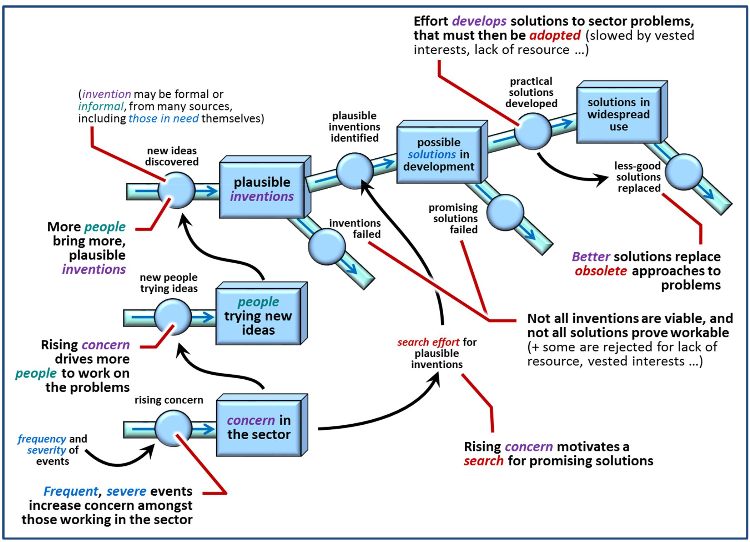
The innovation systems model (see the figure above and on page 30) developed in support of the wider project to which this study belongs defines innovation as passing through several phases:
- Concern in the sector: as the result of, e.g., frequent severe events;
- People trying new ideas: as concern drives more people to look to address particular problems;
- Plausible inventions: as more people bring plausible formal or informal inventions from a variety of sources;
- Possible solutions in development: as plausible solutions are identified and effort is made to develop them; and
- Solutions in widespread use: as practical solutions are made and widely propagated.
At least 5 different types of actors work in emergency infectious disease responses, and they all play a role in the innovation ecosystem. These include: (i) intergovernmental organisations with either wholly or partially health-related mandates; (ii) national governmental organisations operating internationally in the field of infectious disease control; (iii) non-governmental organisations (NGOs); (iv) private foundations; and (v) public-private partnerships and consortia. The case studies span the range of activities undertaken by these actors in humanitarian communicable disease responses with regard to the following 5 areas: (i) diagnostics and assessment; (ii) prevention; (iii) surveillance; (iv) outbreak control; and (v) disease treatment and management. Even though delivery of activities in each of these areas is complicated by emergency contexts, which can serve to limit the possibilities for innovation, some actors in such settings suggest that it is precisely these conditions of emergencies that make innovation so vital because of the potential contribution to saving lives and restoring health.
To cite only one of the case studies offered in the report - that of outbreak control - the positive example is of the Syria polio response, which featured the use of an innovative new outbreak control mechanism (the short interval additional dose approach, or SIAD), in comparison to the relative weakness of the Ebola outbreak control effort. When the ongoing conflict in Syria saw a polio outbreak in October 2013, the first in the country for over 14 years, the initial United Nations Children's Fund (UNICEF) - World Health Organization (WHO) strategy included SIAD as an innovative vaccine delivery approach, having been cited by WHO as a contributor to earlier success in eradicating polio from Somalia. The strategy highlighted the need for multiple doses of the oral polio vaccine (OPV) in short time periods, the mobilisation of community resources (as in Somalia), effective communication messages about the SIAD approach to share with communities, and negotiated access to hard-to-reach populations. This was launched in December 2013....At the time of finalizing this report, the WHO announced that there had been no new cases in Syria for a year, in large part because of the success of the SIAD strategy. The response also saw a unique [WHO-led] event in August 2014, where a number of operational health agencies convened a regional forum during the ongoing response to review innovative strategies for limiting the transmission of polio....A key theme of the meeting deliberations was the use of existing innovations in mapping, surveillance, and control measures, with a particular focus on new medical and communication technologies." In contrast, there were particular failures inherent to the relative novelty of Ebola and its emergence in urban settings for the first time that highlighted the challenge of innovation in outbreak control. "While there were multiple issues around staffing, facilities, and so on, a particular challenge highlighted was the widespread inadequacy of international actors to flexibly respond to changing circumstances with appropriate and relevant strategies."
One section of the paper draws out some of the emerging findings on the nature and condition of the innovation ecosystem in infectious disease responses. For example, though operational humanitarian knowledge is essential at all stages of the innovation process, it is not always well supported or integrated into innovation management efforts. This issue can be seen in the observation, for instance, that the resources made available for furthering knowledge of infectious disease responses in humanitarian crises are frequently for the enhancing the delivery of specific known treatments and protocols. Therefore, when there is funding for research it tends to be for the evaluation of programmes to demonstrate their effectiveness rather than to test new ideas. As Box 1 on Page 30 indicates, there is a good understanding of gaps in evidence, which may also serve a proxy for understanding where evidence-based innovations should be prioritised. However, "[b]ecause of the nature of medical practices and the professional, operational and ethical limits within which it must operate, innovations in disease response are arguably less amenable to improvisation and experimentation than other humanitarian sectors....This focus on medical ethics stands in stark contrast to the almost legitimized lack of regulation of the humanitarian sector as a whole."
This investigation into the innovation ecosystem in humanitarian health suggests that there is:
- a lack of a consistent platform for voicing concerns about humanitarian innovation needs, or an audience that wants to hear these concerns;
- a lack of sustained financing for humanitarian disease innovation processes;
- a lack of methods, protocols, and systems for undertaking trials and a lack of information management and knowledge sharing systems;
- a lack of means or platforms for developing and supporting partnerships for innovation, and a lack of horizon scanning / search and discovery efforts to track the humanitarian relevance of new innovations in the wider global health space; and
- a lack of keystone actors and networks that work to orchestrate and support the ecosystem and hold it together.
On the basis of the above, the paper makes 5 recommendations for how the disease innovation ecosystem might be strengthened:
- More support to stronger innovation leadership, enabling operational organisations to actively work to overcome political barriers to innovation through advocacy and influence work;
- More sustained resources for undertaking design in emergency settings, product horizon scanning, developing research and development (R&D) partnerships, and evaluating approaches - with a greater emphasis on translational research seeking to bring parallel experiments from global health into the humanitarian sector, and more emphasis on simulations to assess viability of new ideas;
- More support for undertaking early stage trials of viable methodologies in disaster settings or equivalent contexts (in part by establishing a common clearinghouse for ongoing trials and experiments);
- More investment in inter-disciplinary partnerships and networks that work across the innovation cycle, ideally developed as neutral platforms where innovation can happen beyond the politics of the sector; and
- Support for a keystone/network role, perhaps by establishing a Global Alliance for Humanitarian Disease Innovation - an international public-private partnership akin to platforms such as GAVI. "This will help elevate humanitarian disease innovation to a global public good."
- Log in to post comments