












































Development of a Culturally and Linguistically Sensitive Virtual Reality Educational Platform to Improve Vaccine Acceptance within a Refugee Population: The SHIFA Community Engagement-Public Health Innovation Programme
University of California San Diego (Streuli, Sawyer); Somali Family Service of San Diego (Ibrahim, Sahid); San Diego State University (Mohamed, Farrell); Palomar College (Sharma); IllumeSense (Esmailian); Distinct Insights (Sezan); The University of Texas Southwestern Medical Center (Meyer); QUALCOMM (El-Maleh); University of Pittsburgh (Thamman); Miami University (Marchetti); Alliant International University-San Diego (Lincoln); University of California San Diego School of Medicine (Courchesne); Healthcare Innovation and Practice Transformation Laboratory (Bhavnani)
"New digital innovations such as virtual reality (VR) have emerged as tools to provide enriching and immersive learning experiences that promote understanding...and ...change health behaviours by engaging users in a non-healthcare environment..."
In the context of decisions about vaccination, refugees can be hampered by a lack of information and/or information that is not culturally and/or linguistically appropriate. Upon resettlement in Western countries, many Somali refugees first learned about autism and were thus vulnerable to anti-vaccination activists propagating the falsehood that vaccines cause the condition. The result has been a propensity for vaccine hesitancy and non-acceptance among this population - for instance, vaccination rates in the Somali refugee population in Minnesota, United States (US) dropped from 92% to 42% over the course of a decade. To combat misinformation, engender trust, and increase health literacy, a group of researchers developed a virtual reality (VR) vaccination education platform with and for a Somali refugee community in San Diego, California, US. This article explains the community-based participatory research (CBPR) models and community co-design approach that ensured the cultural and linguistic appropriateness of the VR platform.
SHIFA (Arabic for "healing") is a community programme to design, deploy, and use new healthcare innovations with an inclusive model of community engagement. For this project, which began in April 2019, SHIFA used CBPR methods, including focus group discussions, interviews, and surveys, to engage 60 adult Somali refugees and 7 expert advisors to design the educational content. Somali community members were involved in the recruitment to the study, as much of the recruitment happened via word of mouth. The researchers consulted with community members and community leaders when designing and conducting the study and developing survey, focus group discussion, and interview questions.
The co-design methodology was inclusive in that community members were asked to participate in content curation and to lead certain aspects of VR development. In brief, the iterative, phased approach to VR development involved:
- Phase 1: CBPR approaches to assess community needs and concerns important to paediatric vaccination - The process began with a series of three focus group discussions and interviews with three Somali parents. Themes that emerged included concerns about autism, medical trust, and the desire to learn more about vaccination. These conversations informed the project team's design workshop, leading to a series of three story ideas for the VR. These ideas were then brought to the Somali community in the form of another design workshop where the community evaluated the suitability of the provided stories and suggested changes.
- Phase 2: VR modality determination for script development - the project team consulted extensively with Somali community health workers (CHWs) to determine an appropriate modality, and chose 360° video due to the ability of this format to be experienced using VR headsets, smart phones, or computers. Somali community members and advisors indicated a preference for a storyline with a strong focus on family and supported the story concept of a Somali mother asking questions to her trusted male physician. Participants in a focus group discussion that assessed this initial script agreed that the VR must address the autism question, and that they would prefer to learn this information from a doctor character in the VR storyline.
- Phase 3: VR prototype and iterative feedback from storyboards, two-dimensional and three-dimensional animation, and visual and audio experiences that incorporate VR design elements, including those factors that allow users to engage at different levels of health literacy - All participants who reviewed the prototype agreed that the inclusion of culturally appropriate characters and a Somali voice-over maximised the educational experience. Thirteen of 24 (54%) participants stated that the prototype made them either more comfortable or much more comfortable with vaccination than they were before exposure to the prototype. Twenty of 24 (83%) participants stated they would recommend measles, mumps, and rubella (MMR) vaccination to members of their community following exposure to the prototype.
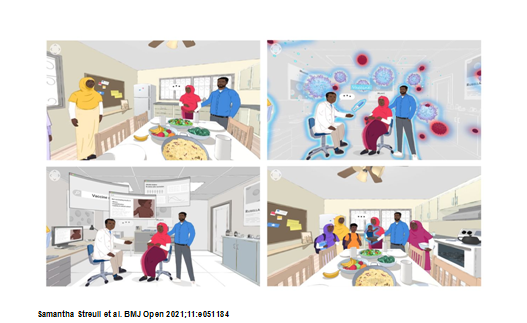
- Phase 4: Final VR product (completed in June 2020 - click on video to watch it, below) and testing (ongoing) - In chapter 1 of the 4-minute animation, the expectant mother, her husband, and her sister visit the doctor's office and learn about MMR. In chapter 2, the family learns how the immune system works. In chapter 3, the family learns from the doctor what the MMR vaccine does and how it works. In chapter 4, the doctor explains to the family the risks and benefits of MMR vaccination, including a statement debunking the association between autism and vaccination. Finally, the 360° video concludes with the new mother, surrounded by her family (including the healthy newborn), stating that after learning all the facts, she has decided to vaccinate her child.
In essence, the researchers carried out a community health assessment and identified the drivers for a low rate of vaccination in the Somali community - ranging from cultural and language barriers, distrust in the healthcare system, and the misinformation that vaccination results in autism. Recognising these drivers for low immunisation rates in this community, their observations for the mechanisms for how VR effects behaviour changes include: content that is culturally relevant, stimulates an awareness and expectation for what vaccines do and do not do, and provides an immersive experience leading to information retention
They note that several design factors must be maintained when considering who interacts with the VR technology, especially among immigrants who may have varying levels of health and digital literacy. Through community co-designs, they leveraged key design factors, including a non-intrusive experience (users learn in their own environment), a passive interaction (content that is visual, audio, and depicted vs reading), and a dynamic storyline that builds on previous experiences, uses known environments, promotes self-reflection by allowing the user to introspect and contemplate during the VR experience, and is culturally and linguistically appropriate - as determined by the community itself.
The researchers plan to develop and leverage an educational curriculum in future deployments of VR. Due to the constraints of COVID-19, they are exploring the possibilities of using telehealth and other digital communication platforms to safely and effectively deploy the VR into the community. There are also concerns about the potential of misinformation related to COVID-19 vaccination that is especially relevant for an underserved community that is largely excluded from vaccine clinical trials and that has a history of vaccine hesitancy. Future research will include an assessment of the efficacy of the VR platform on vaccination rates over time, as well as continued community engagement for the development of additional VR content that can increase health literacy within underserved populations.
In conclusion, the researchers find that a CBPR approach can be effectively used for the co-design of a VR educational programme. Their approach to VR development incorporated community members at each step of the process and is potentially applicable to other populations where cultural sensitivities and language are common health education barriers.
BMJ Open 2021;11:e051184. doi:10.1136/bmjopen-2021-051184.
- Log in to post comments