











































Introduction of Inactivated Polio Vaccine and Specific Determinants of Vaccine Hesitancy
University of Nigeria (Ughasoro, Tagbo); Providence Hospital (Esangbedo)
"There was a wide gap between what parents knew about vaccines and what they were willing to do."
This study was conducted in the context of a strong advocacy effort by the World Health Organization (WHO) for countries using only oral polio vaccine (OPV) to introduce inactivated polio vaccine (IPV), in different combinations with OPV. According to the authors of this paper, "[v]accines in general, whether already in use or newly introduced are faced with the challenge of parental acceptability. The factors that influence the decision by parents or caregivers to allow their children to receive vaccines are enshrouded in complex direct and indirect factors." These factors may include the fact that IPV is delivered as an injection, with the associated injection pain and complications of injection, which may make IPV more subjective to parent vaccine hesitancy.
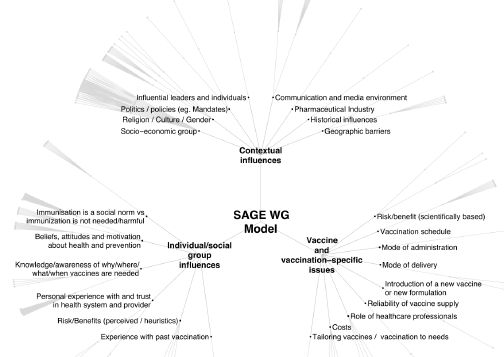
Participants in the study were parents who brought their children for immunisation at the University of Nigeria Teaching Hospital, Enugu, and Federal Medical Centre, Umuahia. Random systematic sampling based on the daily immunisation attendance register was used to select parents. The questionnaire, adapted from the model developed by the Strategic Advisory Group of Experts Working Group (SAGE WG) - see Related Summaries, below - was used to assess the factors for vaccine hesitancy among 408 parents. The evaluation was conducted under the 3 Cs: Confidence, Complacency, and Convenience. Questions were scored on the Likert 4-unit-scale system. The data were analysed using the Statistical Package for Social Sciences (SPSS), and multivariate analysis was used to further test individual significant variables.
An excerpt from the document reporting results follows: [footnote numbers have been removed]
"Most [of the parents who participated in the survey] believed that vaccines can cause adverse events, lack knowledge on vaccine content and were not confident that the vaccinators are competent enough to execute their duties. But they were still willing to allow their child to be vaccinated with IPV. This is in keeping with the report that even without adequate vaccine knowledge; most parents will still vaccinate their children. Introduction of IPV shares the contextual influences of both an existing vaccine and an entirely new vaccine, while previous vaccine hesitance studies have been on vaccine hesitancy to already available vaccines. There is a potential of vaccine hesitancy towards IPV when introduced and OPV is still retained in the immunization schedule, especially if the clinical reasons behind introduction of IPV are not adequately disseminated to the people.
The proportion of parents who were hesitant to vaccinate their children with IPV if OPV is still retained in the immunization schedule was high, but not significant. This means that though parents still prefer OPV, they will reluctantly accept IPV once approved by the ministry of health even if OPV is still retained as an option. Studies have shown that with the right information, and adequate awareness creation and availability of new vaccine, parents vaccinate their child with newly introduced vaccine. Therefore, with adequate information and awareness creation, parents will accept IPV, although the extent of their acceptance will be influenced by other factors such as whether IPV will be included in publicly funded vaccines...
Most of the responses given by the parents were pro-vaccine hesitancy, but [the] majority still accepted to vaccinate their children. This highlights the lack of connection between their understanding of various aspect of vaccination and their intended actions. Nonetheless, the fact that all the recruitment of participants in the study took place in immunization clinics indicate that the parents are likely to be pro-vaccine oriented, and may not be representative of the entire community. Normally, parents are given [a] health talk at the immunization centers before administering vaccines. Therefore they are more exposed to the benefits of vaccination, and irrespective of the barriers and challenges, they are relatively empowered to act in a pro-vaccine manner. This may be a possible explanation of why a proportion of parents willing to vaccinate their children with IPV did not change much irrespective of their response to item questions. This further highlights the impact of health education on vaccine acceptance. Relatively equal proportion of the respondents held negative and positive attitudes towards the different aspects of vaccination program. However, majority were strong on their intention to vaccinate their children with IPV. This could be due to the already established parents' disposition to accepting any health related intervention, provided it is presented in a health facility.
The proportion of the parents that believed that their children will not contract poliomyelitis even if not vaccinated was low. It is still worrisome that some parents still harbor such belief...
A major limitation of this study was not including a community evaluation to get opinion of those that will utilize immunization services in the future....The respondents involved in this study were mainly urban dwellers, fairly educated and mostly Christian, which may not be a good representation of the overall Nigerian population. However, regional or small unit evaluation is very helpful in the development of an intervention that brings indigenous solution rather than evaluation at the national or global level..."
The lack of trust on the competence of health care providers involved in [the] immunization program by the parents as reported in this study should be explored further..."
World Journal of Vaccines, 5, 8-18
- Log in to post comments