












































Scared, Powerless, Insulted and Embarrassed: Hesitancy Towards Vaccines among Caregivers in Cavite Province, the Philippines
Research Institute for Tropical Medicine (Landicho-Guevarra, Reñosa, Endoma, Aligato, Bravo, Landicho); Ruprecht Karls Universität Heidelberg (Reñosa, Wachinger, Bärnighausen, McMahon); University of the Witwatersrand (Bärnighausen); Johns Hopkins University Bloomberg School of Public Health (McMahon)
"...caregivers' childhood vaccine refusal and delays on individual and interpersonal levels are mostly anchored in past experiences and resulting fears..."
There is a paucity of data from low- and middle-income countries (LMICs) describing the reasons why parents or caregivers refuse or delay childhood vaccinations (vaccine hesitancy, or VH). Thus, this study presents insights from vaccine-hesitant caregivers (VHCs) in the Philippines, an LMIC where a large-scale, highly politicised vaccine controversy has resulted in declines in vaccine confidence.
In the 2017 Dengvaxia case, rumours and fear narratives (such as unverified claims about child deaths) rampantly spread on social media platforms, creating social divisiveness and public tension. The Philippines, where a majority of the population in urban and rural areas accesses the internet and use social media, is a promising case study to investigate individual vaccination narratives and barriers.
Conducted as part of a larger mixed methods study (Project SALUBONG), the research draws on in-depth interviews (IDIs) conducted online (e.g., via Zoom or Skype) between August 2020 and March 2021 with 44 VHCs in rural and urban communities in Cavite Province, the Philippines. (From 2018 to 2019, the Calabarzon region saw a 300% increase in measles cases.) The researchers analysed the qualitative data drawing from the tenets of constructivist grounded theory (CGT), and use the social ecological model (SEM) to structure the results.
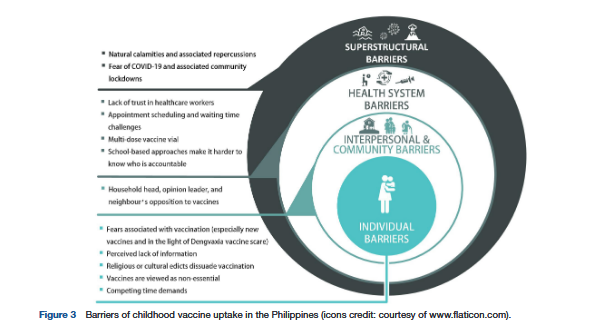
Main barriers include:
- Individual level
- Fears associated with vaccination (especially new vaccines and in the light of Dengvaxia vaccine scare) - Such concerns were the most salient, especially based on things their children experienced or "horrible stories and videos" (Mother of 7, age 46) they had heard and watched. Respondents cited the dengue vaccine controversy as they expressed reluctance (regarding any new vaccines) and suspicion (towards school-based vaccination, the distribution channel used for the dengue vaccine).
- Perceived lack of information - Several respondents reported they had not received detailed information on the recommended vaccines by healthcare workers (HCWs) - for example, regarding what to do in instances when a child may experience adverse events, especially in light of reports of suffering associated with Dengvaxia.
- Perception that vaccines are non-essential - Respondents felt vaccines were only used by a tiny minority when they were young, and that nevertheless the non-vaccinated majority grew into healthy adults.
- Competing time demands.
- Interpersonal and community barriers: Household heads', opinion leaders', and neighbours' opposition to vaccines - For example, respondents, particularly mothers, said they had to defer to heads of households (husbands, mothers-in-law), and that this person routinely opposed vaccination because they believed it harms children.
- Health system barriers
- Lack of trust in HCWs - Most respondents stated they saw their vaccination-related questions as valid, considering that the health of their children was at stake, but were insulted, hurt, and/or embarrassed by the HCWs' reactions. The perception of HCWs as dismissive, unavailable, or disrespectful in terms of answering questions or concerns about vaccines leads caregivers to rely more heavily on other channels for information, such as their own social circle or social and traditional media. However, these channels can function as "echo chambers", wherein caregivers are repeatedly confronted with heavily biased information. Some respondents also shared instances when they forgot or lost their vaccination cards and were afraid that HCWs would scold and shame them, as previously experienced by themselves or other parents.
- School-based approaches that make it harder to know who is accountable - Parents felt left alone with their questions and were unsure who would be responsible after learning about the potential side effects.
- Appointment scheduling and waiting time challenges
- Superstructural barriers included: natural calamities that can complicate travel to a health centre, and fear of COVID-19 and associated community lockdowns. As an example of the latter, respondents also shared fears regarding how vaccines, namely polio, were being administered by HCWs amid the pandemic. Respondents explained how the polio vaccine is commonly packaged in small plastic vials from which HCWs squeeze the vaccine directly into the child's mouth, which is perceived as risky, especially in times when the SARS-CoV-2 virus is widespread. In addition, respondents viewed house-to-house polio and measles vaccination campaigns as unhygienic.
In reflecting on the findings, the researchers note that the prominent role of fears resulting from the Dengvaxia controversy among the VHCs they interviewed highlights the need to further explore how vaccine scares can shape narratives about vaccines and health systems. These results "highlight how the mental trauma of vaccine scares remains within the family and has profound and persistent effects, which has also been described in the Philippines and elsewhere in relation to fears brought by misinformation to vaccine."
Another avenue for future research could be investigation of the ways in which power is exerted by household members and other stakeholders in vaccination decision-making processes. Such data could provide insights that allow for the development of interventions that are geared toward the different decision-makers, while acknowledging the interplay between the various role-specific socioecological factors.
The researchers also cite some of the (considerable amount of) literature that highlights pathways for interventions to regain trust and bolster confidence in vaccines. For example: "Risk communication skills that allow for rebuilding trust and transparent and clear health education campaigning aimed at VHCs would be of great importance for reviving vaccine uptake...."
In conclusion: "Various strategies and policies to cope with past and current vaccination challenges to bolster vaccine uptake are needed to address individual concerns of VHCs at the centre of any intervention."
BMJ Global Health 2021;6:e006529. doi:10.1136/bmjgh-2021-006529. Image (icons) credit: courtesy of www.flaticon.com
- Log in to post comments