











































Measuring Vaccine Confidence: Introducing a Global Vaccine Confidence Index
London School of Hygiene and Tropical Medicine (Larson, Schultz, Smith); University of North Carolina at Chapel Hill (Tucker)
"The prevention of vaccine-preventable disease outbreaks, such as measles, rubella, or polio, is dependent on herd immunity. Yet ensuring widespread vaccination coverage is complicated by a wide range of factors, including vaccine hesitancy, which causes uncertainty in segments of the public about the safety and efficacy of vaccinations."
This article presents the findings of a multi-country survey of confidence in vaccines and immunisation programmes in Georgia, India, Nigeria, Pakistan, and the United Kingdom (UK). These are the first results of a larger project to map vaccine confidence globally. The authors explain that people may lack confidence in the safety or efficacy of vaccines as a result of negative experiences with the product, providers, or those making the policy decisions. They may hold religious or philosophical beliefs that lead them to prefer traditional rites, prayers, or homeopathic remedies over biomedical interventions. And, yet: "Vaccine confidence is not merely an individual phenomenon, but a social and political phenomenon as well. When vaccine-hesitant individuals reach a critical mass in a population, and do not receive adequate attention and engagement from health authorities on the specific issues they may have with a vaccine, they may form coalitions of varying looseness or consensus....Vaccine confidence metrics can provide valuable cues to changing public sentiment about vaccines and the potential for consequent changes in vaccine coverage.....Measuring vaccine confidence is an emerging science. In developing our Vaccine Confidence Index (VCI), we have taken cues from other social science tools that measure confidence more generally....The VCI can likewise be a potentially useful tool for researchers and policy-makers, and could provide an empirical basis for monitoring vaccine confidence over time in a number of regions."
"The five countries chosen for the initial launch of the Vaccine Confidence Index have each faced a confidence crisis, and they have addressed these confidence challenges with differing levels of success." For example, in Nigeria in August 2003, a polio vaccination boycott was announced in 5 northern states and persisted in Kano State for 11 months, only being resolved in July 2004. The India polio programme also encountered distrust, including similar rumours of sterilisation, among marginalised and underserved communities in the states of Uttar Pradesh and Bihar. "Years of targeted efforts to build trust and confidence, in the vaccine as well as in the polio programme as an institution, were key contributors to India's being declared polio free a decade later in January 2014."
Data were collected in 2014 from a sample of the general population and with respondents with children equal to or under the age of 5 (RCU5), against a core set of confidence questions, communicated in the local language. Methods included: face-to-face in-house interviews (Pakistan), online interviews (UK), computer-assisted telephone interviewing (India), face-to-face interviews (using personal digital assistants [PDAs]) and health provider interviews (Nigeria), and computer-assisted personal interviewing (Georgia). The researchers examined: confidence in immunisation programmes as compared to confidence in other government health services, the relationships between confidence in the system and levels of vaccine hesitancy, reasons for vaccine hesitancy, ultimate vaccination decisions, and their variation based on country contexts and demographic factors. The numbers of respondents by country were: Georgia (n=1,000), India (n=1,259); Pakistan (n=2,609), UK (n=2,055), Nigerian households (n=12,554), and Nigerian health providers (n=1,272).
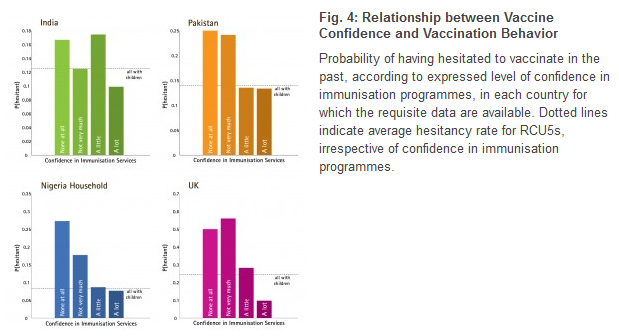
Reported reasons for hesitancy in all countries were classified under the domains of "confidence", "convenience", or "complacency", and confidence issues were found to be the primary driver of hesitancy in all countries surveyed. (As Figure 4 illustrates, confidence is a sentiment linked to behaviours of hesitancy and refusal.) The results show that UK RCU5s were more likely to hesitate to vaccinate, compared to other countries. Using the Spearman rank correlation coefficient, which assesses how well the relationship between two variables can be described using a monotonic function, the researchers found that confidence in immunisation programmes was more closely associated with confidence in the broader health system in the UK (ρ=0.5990), compared to Nigeria (ρ=0.5477), Pakistan (ρ=0.4491), and India (ρ=0.4240) - all of which ranked confidence in immunisation programmes higher than confidence in the broader health system. Georgia had the highest rate of vaccine refusals (6%) among those who reported initial hesitation. In all other countries surveyed, most respondents who reported hesitating to vaccinate went on to receive the vaccine except in Kano state, Nigeria, where the percentage of those who ultimately refused vaccination after initially hesitating was as high as 76%. Meanwhile, Nigerian health providers' high confidence ratings for all services resulted in this group of respondents showing the strongest associations between confidence in the immunisation programme and confidence in all other services, compared to the confidence expressed by the general public in any of the countries surveyed.
In conclusion, the authors note that "medium-to-high confidence in vaccines and immunisation programmes is the norm, and vaccine hesitancy and refusals are relatively rare. Nonetheless, even small groups of hesitant or refusing individuals can severely undermine an immunisation programme in certain circumstances, such as when political actors in Nigeria and Pakistan mobilised local boycotts that have had both national and international repercussions." They reiterate that higher confidence in immunisation programmes correlates with lower vaccine hesitancy and lends support to the premise that confidence in vaccination is connected to confidence in the broader system with which it is associated. They pose the question: "How much confidence is enough?" - which, at the societal level, for example, leads to further questions, such as: "[I]s there a critical proportion of the population that must remain vaccine-confident for the system as a whole to remain resilient to a 'crisis of confidence,' in which doubt becomes prevalent enough that it becomes self-reinforcing? Is there a crucial point beyond which previously-confident laypersons begin questioning the vaccine, healthcare providers become less willing to promote it, and policy-makers consider withdrawing a recommendation for an effective and safe vaccine for fear of public disapproval? Is it more dangerous if a small part of the population to lose a great deal of confidence, or if a larger group becomes only slightly less confident? And, again, what contextual factors heighten the risk of a crisis at any given level of vaccine confidence?"
They say that answering these questions will require data gathered from multiple countries, over time, through efforts such as this global vaccine confidence mapping initiative. "In effect, we are attempting to launch a large cohort study of as many countries of the world as possible. If the cohort is large enough, and the timescale is long enough, then it will become possible to relate 'incident cases' of vaccine confidence crisis to the 'exposures' measured through surveys of confidence and relevant contextual and demographic factors, permitting ascertainment of the 'risk factors' for crises with both quantitative rigour and qualitative depth."
PLOS Currents: Outbreaks collection, accessed November 24 2015.
- Log in to post comments