











































Vaccine Hesitancy as a Challenge or Vaccine Confidence as an Opportunity for Childhood Immunisation in India
GSK (Agrawal, Kolhapure, Di Pasquale, Ray); private practitioner (Mathur)
"To address the problem of VH in India, there is a need to estimate its root causes, formulate context-specific strategies relevant to the local settings and thus help in restoring trust leading to increased confidence in vaccination."
India, where 27 million children are born each year, has not been able to reach the goal of 90% coverage for all vaccines included in the national immunisation schedule because of various factors, including vaccine hesitancy (VH). The objective of this qualitative literature review was to identify: the set of VH determinants impacting childhood immunisation in India, key challenges to overcoming reluctance to vaccination in the country, and opportunities to minimise VH in India and increase confidence around vaccination.
A search for relevant literature published between 2015 and 2019 led to 9 articles reporting childhood VH determinants in India. Selected findings:
- Social connections affect attitudes towards vaccination, as seen during an oral polio vaccine (OPV) campaign. Among the 1,355 households with one or more children under 5 years old, 137 were hesitant (10.1%), and 144 (10.6%) refused vaccination. Vaccine-refusing households had 189% more ties to other vaccine-refusing households than to vaccine-accepting households, which shows a clustering of VH communities.
- Social relationships and access to information through social media had an impact on uptake of measles-rubella (MR) vaccination. Vaccine acceptance was higher when offered at school (P<0.001). It was also high among parents who trusted school teachers (P<0.003) and other school children (P<0.014) as sources of information. However, acceptance was lower among parents who trusted information from social media (P=0.036).
- In another study, 14.1% of the 461 parents of children between 9 months and 15 years old were hesitant towards the MR campaign. VH was more prevalent in parents with less education (P=0.04) than in those who had graduated. Major hindering factors were inadequate knowledge about the vaccination campaign, rumours about the safety of the vaccine, sudden planning, and under-preparedness at the health system level. A major facilitating factor for the campaign was the role played by healthcare professionals (HCPs) in spreading awareness and increasing trust in vaccines and vaccination.
- In a study finding that only 17% (33/194) of the children under 5 years old in households located in the slums of Siliguri had received vaccinations on time, 20.5% cited unawareness/receiving no reliable information as a reason for VH.
- A comparison of VH across 5 low- and middle-income countries (LMICs), made using the World Health Organization (WHO)'s 10-item VH Scale, included VH data for India from 309 mothers of children under 5 years old. The majority of the hesitant mothers were concerned about safety (39.2%), believed some vaccines were no longer needed (33%), or feared that newly introduced vaccines could threaten children's health (20%).
- In 2018, interviews at a tertiary care centre of 150 mothers of children 1 to 5 years old revealed that suspicions towards newer vaccines (61.4%), concerns about adverse events (90.7%) and perception that vaccines are not necessary for uncommon diseases (85.3%) were related to hesitant behaviour as measured by the vaccine confidence index. Mother's education was seen to protect against VH, whereas father's education, father's use of social media, and reliance on sources of information other than a HCP increased the risk of VH.
- Ten Indian paediatricians interviewed for a qualitative survey conducted among 75 HCPs from 4 countries in 2018 reported that vaccine costs and shortages were important challenges in India. They also cited lack of general understanding about the purpose of vaccines in segments of the population.
- A questionnaire based on that created by the WHO strategic advisory group of experts on immunisation was administered to 260 households in Odisha. Nearly 28% and 9% of parents in Balangir and Nuapada, respectively, had heard negative information about the vaccines. Still, over 75% of them had their children vaccinated.
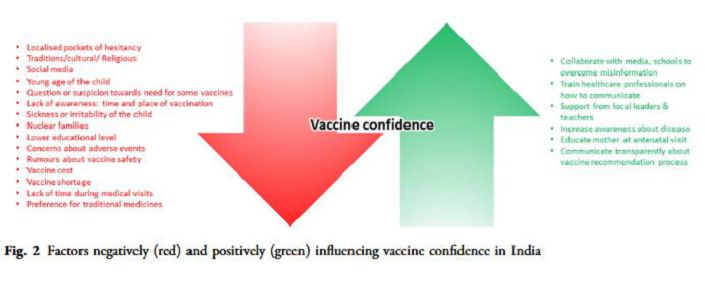
These results suggest many challenges surrounding vaccination in India, some of which are particularly prominent because of their impact or shared roots with broader health issues. They include:
- Rumours and controversies - For instance, during poliomyelitis vaccination programmes in early 2000, a seed of distrust was sown in particular communities by linking vaccination with sterility and by falsely claiming that pigs' blood was present in the vaccine, among other things. However, realising the importance of vaccination, religious leaders who were silent initially, along with community influencers, eventually actively fostered the social mobilisation that led to the successful elimination of poliomyelitis. Another example: Safety concerns were raised after the deaths of 7 girls during 2 human papillomavirus (HPV) vaccine studies conducted in 2010. Though an investigation concluded that the vaccines were not responsible for the deaths, and despite recommendation by the Indian Council of Medical Research and the National Technical Advisory Group on Immunisation, the call for introduction of HPV vaccine is still opposed.
- Social interactions - Behaviour with respect to vaccination tends to depend on whom you know, where you live, or both. For example, low uptake of the MR vaccine (44% of the targeted number of children) during the 2017 vaccination campaign in Tamil Nadu reflects the hesitant behaviour of parents associated with safety concerns that are usually spread through social interaction and media.
- Healthcare system and access to facilities - India has various geographical features with areas that are either densely or sparsely populated. Results from pooled, nationally representative surveys covering 1998-2008 evidenced that lack of access to immunisation facilities, along with absence of healthcare workers and ignorance of the place and timing for getting vaccination, were among the reasons for delayed or missed vaccination. To look at one of those factors in more detail: Inadequate workforce increases the pressure on healthcare workers and may lower their availability to discuss parents' concerns regarding vaccination. Previous negative experience with HCPs was indeed reported as one of the reasons for VH, and healthcare workers' lack of empathy in slums (possibly due to elevated workloads) was perceived as a barrier in the immunisation process.
- Economic factors - Very few vaccines are offered free or as part of the national immunisation programme.
- Vaccine-specific challenges - For example, suspicions towards newly introduced vaccines, as well as doubts about the need to vaccinate against diseases that are uncommon, are recurrently reported in the Indian population.
Tailoring immunisation programmes has proven to be efficient to address gaps in vaccine uptake among a population, notably by addressing VH. Some opportunities to increase vaccine confidence in India include:
- Communication - Today, access to social media (72.9% of households use smartphones) is far greater in India than access to cooking gas cylinders. Usually, mothers seek information online, especially when concerned about vaccine safety. As it is difficult to control and verify all the information available on the various platforms, it is important to increase access to transparent and scientifically validated information about the risks and benefits of vaccines, as well as to answer questions with balanced and accurate information. Healthcare workers have been found in various studies to remain the most trusted advisors among all possible sources of reliable information when it comes to vaccination. The situation in LMICs is even more closely impacted by healthcare workers (including community health workers, Anganwadi workers, auxiliary nurse midwifes, and health assistants), as they represent the frontline of vaccination and are often confronted with questions from hesitant parents. Therefore, communication training of healthcare workers appears to be a promising strategy for dealing with VH and improve vaccine confidence. For example, applying the CASE (Corroborate, About Me, Science, and Explain/Advise) approach could help them establish a dialogue with parents. Furthermore, this approach could reinforce the impact of self-help groups that are already shown to improve healthcare access and awareness in rural communities. Similarly, religious leaders could be included as partners when communicating about immunisation. For example, the mobilisation of Muslim leaders in India was instrumental in the eradication of poliomyelitis.
- Education and creating awareness about immunisation and fostering critical thinking on associated risks and benefits - For example, including a basic curriculum on vaccine-preventable diseases (VPDs) in schools could have a positive impact in the long term by making the new generation aware of vaccination's risks and benefits (e.g., HPV). Moreover, school teachers are recognised as a trustworthy source of information by parents accepting vaccination. Schools and school teachers also have the potential to dissipate cultural barriers, which are a deterrent to vaccination.
- Efforts to address safety concerns - For example, nurturing and using the national surveillance programme of adverse events following immunisation (AEFIs) is important for building evidence about vaccine safety and assuring the public that continuous monitoring is in place to help assessing any suspicion of a safety issue.
Thus, the proposed strategies include: involving local stakeholders; encouraging the use of different mass media techniques to increase awareness of risks and benefits and address the prevalent myths about vaccines and vaccination; improving convenience and accessibility to the vaccines; employing reminder and follow-up services; organising training sessions for healthcare workers to enhance their communication skills and ability to engage in balanced and scientifically validated dialogues with parents; and providing nonfinancial incentives to immunised individuals. "The success of the polio campaign that helped in its elimination in India can be attributed to all the above factors and could serve as an example for overcoming challenges in vaccination."
Infectious Diseases and Therapy (2020). https://doi.org/10.1007/s40121-020-00302-9
- Log in to post comments