











































Critical Interventions for Demand Generation in Zambia, Nepal, and Senegal with Regards to the 5C Psychological Antecedents of Vaccination
Emory University (Hester, Sakas, Ogutu, Ellis, Yang, Freeman, Orenstein, Bednarczyk); Center for Molecular Dynamics Nepal (Dixit); Center for Family Health Research in Zambia (Chanda); Institut de Recherche en Santé de Surveillance Epidemiologique et de Formation - IRESSEF (Sarr)
"Categorizing interventions by what drives demand may support strategic planning and influence the division of resources."
The 5C psychological antecedents of vaccination ("5C") model provides a validated measure of vaccine hesitancy or confidence that is used to assess individual thoughts and behaviours behind vaccination. The five components of the 5C model include confidence, complacency, constraints, calculation, and collective responsibility. This study investigated population-level factors that contributed to high and sustained vaccination coverage in Zambia, Nepal, and Senegal, and alignment with the 5Cs.
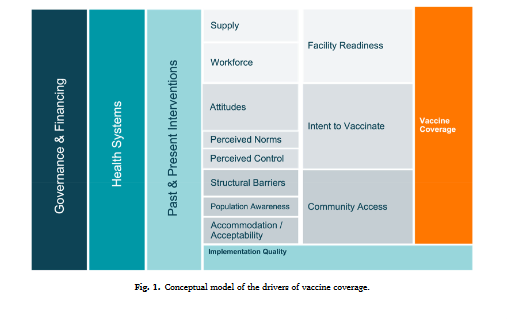
Prior to data collection, the researchers developed a conceptual model (above) to organise factors that impact childhood vaccine coverage globally. While components of vaccine demand and intent are present in this model, they sought the use of the 5C model to further assess the demand environment of the selected countries.
Data were collected between October 2019 and April 2021 as part of the larger Exemplars in Vaccine Delivery study, more information about which is available at Related Summaries, below. Methods included focus group discussions (FGDs) and key informant interviews (KIIs) at the national, regional, district, health facility, and community levels of health systems in Zambia, Nepal, and Senegal. The researchers assessed the demand environment, as relayed by participants, and identified interventions reported as successful for demand generation, then retroactively aligned the interventions with the 5C constructs.
Overall, the study found that the 5Cs were an effective way to analyse intent and demand generation within the studied populations. Collective responsibility was the construct most correlated to demand generation in these countries. All studied countries exhibited cultural norms that related to collective responsibility, with participants from the community and health sector alike stressing the importance of the collective health of their communities. Although collective responsibility was the most prominent construct seen across the countries, interventions that utilised this construct may be the most difficult to replicate due to differences in culture and values.
Key informants from all three countries reported high levels of intent to vaccinate and demand for vaccine among their communities. Demand was positively correlated with high confidence and collective responsibility. Factors often negatively correlated with vaccine intent, such as complacency and calculation, were limited in impact in these three countries.
Not all constructs were directly transferrable at a population level as currently described in the 5C model. For example, population-level demand had improved alignment with constraints once the researchers separated it into two subcategories: physical constraints and psychological constraints. When looking at physical constraints separately, they determined that for some communities, access did not affect demand; in fact, parents' demand for vaccines was high enough to make physical barriers, such as traveling long distances or waiting long periods, worth pressing through to protect their children from diseases. They theorise that this difference may be explained by the low- and middle-income country (LMIC) status of Nepal, Senegal, and Zambia, and they recommend that further use of the 5C model in LIC/LMIC settings have the constraint construct separated into these distinct sub-categories.
Similar interventions across countries were used to generate demand, and these interventions ultimately aligned with all constructs of the 5C model. The exemplar countries addressed community vaccination behaviour within all constructs through interventions including:
- Targeted and tailored health education activities: For example: Confidence in vaccines was fostered through dissemination of accurate and timely information from trusted sources; collective responsibility was maintained by filtering vaccination messaging through societal norms and cultural ties; complacency was addressed by education of parents and children on immunisation and danger of infectious disease; psychological constraints were addressed by providing media with tools to address misinformation and hesitancy along with information about upcoming vaccination events; and calculation was dissuaded by media and government transparency along with easy access to accurate information.
- Media partnerships: Within the Ministry of Health (MoH) in all three countries, there were designated governmental agencies that handled media engagement. Countries utilised these partnerships to disseminate accurate information to communities, ultimately fostering trust in both the government and vaccines. At the local level, information was shared a variety of ways - radio being the most prevalent. Each country had unique modalities for media dissemination, such as an online news portal (Nepal), peer-to-peer learning from recorded visits (Zambia), and press caravans - defined as small-scale campaigns (Senegal).
- School outreach: The education systems in these countries were used to promote vaccination among children - either directly or indirectly.
- Community engagement and ownership of health interventions and outcomes: Across all sites, respondents spoke to the importance of community actors for the implementation of demand generation activities, including their input on messaging and support for outreach. The MoH leveraged partnerships with community leaders, religious leaders, traditional leaders, and community health workers (CHWs) to increase vaccine demand and uptake. Interventions related to community ownership also aligned with the other antecedents for demand by: creating confidence in vaccines and service providers through the existing respect and trust of volunteer CHWs; addressing psychological constraints through tailored activities to local areas and individualised outreach to parents; addressing complacency by increasing public awareness through community channels; and limiting the impact of calculation through proactive engagement with community members and dissemination of accurate information.
- CHWs: These personnel are influential players within the healthcare systems of Zambia, Nepal, and Senegal. For example, in Nepal, female community health volunteers (FCHVs) are the main sources of vaccination information in communities. FCHVs are recruited to work in their own communities and utilise knowledge of community values, norms, and priorities to adjust messaging and personal communication to address the needs of specific groups. FCHVs ensure community members are knowledgeable of their right to receive vaccines and engage directly through door-to-door education. Similarly, in Senegal, CHW cadres called relais and bajenu gox ("godmothers") sensitise communities several days before vaccine days and check vaccination cards to assess whether children needed to attend upcoming events. In some cases, they call or texted parents to remind them of vaccination days. These CHWs provide extensive follow-up on dropouts, including door-to-door activities, and encourage reluctant parents to vaccinate their children. Zambia utilises neighbourhood health committees to dispel myths and misconceptions about vaccinations.
- Community leaders, organisations, and religious figures: In all three countries, involvement from community leaders and community-based organisations was seen as critical to connect communities to the healthcare system, and community actors acted as gatekeepers to their communities. To cite only one example, Zambia has been particularly successful at leveraging social civil society organisations like the Churches Health Association of Zambia to help increase trust and participation in the immunisation programme. These organisations assist by providing information about vaccination programmes and dispelling myths.
Based on their work in Zambia, Nepal, and Senegal, the researchers recommend the following strategies to target all 5C constructs and improve population-level demand:
- Utilise existing community structures, and consider cultural and social norms when designing interventions.
- Disseminate vaccine information through multiple trusted sources, such as CHWs, newspapers, radios, and religious leaders.
- Conduct school outreach by providing schoolteachers with lesson plans on health, including the importance of vaccination.
- Assess physical and psychological constraints separately in low-income country (LIC)/LMIC settings, and respond to each via tailored programming.
In conclusion: "Assessing the 5Cs allows decision-makers to operationalize demand generation into concrete interventions and policies, and determine the individual impact of these constructs on the population and focus efforts on interventions tailored to a specific need."
Vaccine: X 14 (2023) 100341. https://doi.org/10.1016/j.jvacx.2023.100341.
- Log in to post comments