











































Internal and External Factors Affecting Vaccination Coverage: Modeling the Interactions between Vaccine Hesitancy, Accessibility, and Mandates
"Understanding local vaccination cultures, which evolve through an interaction between beliefs and behaviors and are influenced by the broader cultural landscape, is critical to fostering public health."
An increase in vaccine hesitancy, an individual mindset informed within a cultural context, has resulted in a decrease in vaccination coverage and an increase in vaccine-preventable disease (VPD) outbreaks. Local vaccination cultures - the shared beliefs among individuals within a community about vaccine-preventable disease etiology, prevention, and treatment - can affect an individual's vaccine attitudes and decisions. Cultural niche construction theory describes a process in which humans modify their cultural environments - for example, their beliefs, behaviors, preferences, and social contacts - in ways that subsequently alter evolutionary pressures on the population and its culture. By using this type of model to simulate the interactions between beliefs and behaviours, this paper seeks to understand how vaccination cultures affect vaccination coverage, as well as how vaccine-related beliefs and behaviours are affected by external forces, such as the availability of vaccines and the degree to which they are mandatory.
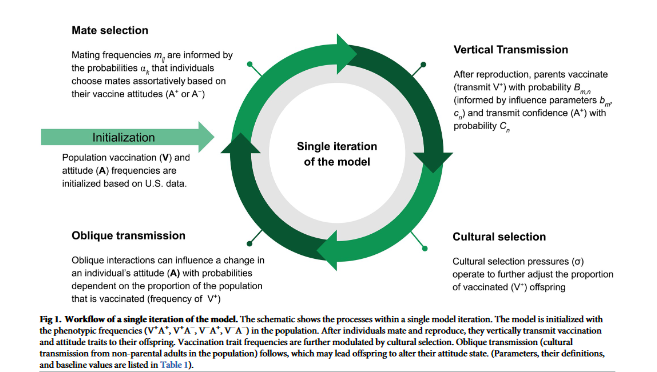
For a population of individuals, the researchers track the status of vaccination coverage and vaccine confidence over time; within this population, individuals mate, decide whether to vaccinate their offspring, and transmit a vaccine attitude trait. Each individual in the model has a vaccination (V) trait, either V+ (vaccinated) or V- (unvaccinated), and an attitude (A) trait, either A+ (vaccine confident) or A- (vaccine hesitant), resulting in four possible phenotypes (V+A+, V+A-, V-A+, and V-A-). To model the effects of the external factors, the researchers assume that vaccine mandates and inaccessibility both act to reduce the influence that internal factors, such as individual beliefs, have on vaccination behaviours.
Modeling the effects of a vaccine mandate reveals a decoupling of vaccination coverage and vaccine confidence trajectories when parents are more likely to transmit vaccine hesitancy to their offspring. Even when vaccine confidence is very low, vaccination coverage is higher with a less strict mandate implemented than without a mandate. However, a more lenient mandate means that many vaccine-hesitant couples can obtain an exemption, and vaccination coverage remains lower when vaccine hesitancy is common. This scenario suggests that an external pressure to vaccinate helps overcome the opposing cultural pressure imposed by hesitancy in the population, but a mandate would have to be stricter to achieve herd immunity in a predominantly vaccine-hesitant population.
Juxtaposed with the mandate scenario, the vaccine scarcity models produce an opposite deviation of vaccination coverage from vaccine confidence levels: When vaccines are mandated, the researchers observe increased vaccination coverage in low-confidence environments, and when vaccines are inaccessible, they observe lower than expected vaccination coverage (<50%) in a predominantly vaccine-confident environment (>90%).
In summary, compared to baseline outcomes, implementation of a mandate increases vaccination coverage at the expense of confidence by driving vaccination in hesitant individuals, and vaccine inaccessibility promotes confidence despite low vaccination coverage by driving confidence in unvaccinated individuals.
When mixed-attitude couples transmit confidence to their offspring at high or low probabilities, which skews population attitude frequencies to either highly confident or highly hesitant, the subsequent offspring are more likely to vaccinate (in a confident population) or not vaccinate (in a hesitant population).
In short, when there are external pressures as modeled here, such as increased pressure to vaccinate or difficulty in acquiring vaccination exemptions, an undercurrent of vaccine hesitancy can persist in a relatively well-vaccinated population, potentially limiting the adoption of newly introduced vaccines. This possibly contributes to the unexpected lag in uptake of newer vaccines, such as the COVID-19 or human papillomavirus (HPV) vaccines, in communities with otherwise high vaccination rates. The perceived increase in hesitancy surrounding new vaccines may actually be existing vaccine hesitancy becoming apparent. In addition, "fence sitters", who have not made a firm stance regarding vaccines and thus could be more influenced by targeted campaigns, may develop higher levels of uncertainty about new vaccines than their parents had about existing ones.
By modeling vaccine inaccessibility, the researchers illustrate another pattern: reduced vaccination coverage in a vaccine-confident culture. In a vaccine-scarce environment, an individual's attitude regarding vaccines has less influence on vaccination behaviour due to the barrier imposed by resource availability. As a result, a population may be undervaccinated despite holding vaccine-affirming beliefs. In addition, a health culture previously shaped by vaccine inaccessibility could potentially ingrain specific behavioural practices (for example, visiting the doctor only when a child is sick and not for a regular vaccine schedule) that are not easily modified even if vaccines become more readily available. These vaccine scarcity scenarios are most likely to exist in low- and middle-income countries (LMICs), whereas the opposite scenario (low vaccine confidence-high vaccination coverage) after vaccine mandates is most common in developed nations.
This paper has shown that vaccine mandates can result in high vaccination coverage even in a culture of hesitancy, and that lack of access to vaccines can produce the inverse: low vaccination coverage in a culture of confidence. The model shows, in both mandate and inaccessibility scenarios, that the probability of transmitting vaccine-positive attitudes is a strong predictor of whether future vaccination coverage is high or low. Thus, the model "demonstrates the importance of clear and accurate communication about vaccines even when vaccination is mandatory and resulting coverage is high, to reduce the spread of inaccurate information that can foster vaccine hesitancy and hinder the uptake of future vaccines. Taken together, the results...suggest that combatting low or declining vaccine uptake would take a sophisticated approach that targets the physical vaccination behavior (availability and mandates) while simultaneously addressing a population's constantly evolving vaccine perceptions."
PLOS Global Public Health 3(10): e0001186. https://doi.org/10.1371/journal.pgph.0001186.
- Log in to post comments