











































Vaccination Hesitancy: An Overview
Centre de recherche du CHU de Québec (Dubé); Institut national de santé publique du Québec - INSPQ (Dubé); Université Laval (Dubé); Université de Sherbrooke (Laberge, Guay); Centre de recherche du CSSS Champlain-Charles-LeMoyne (Guay); Direction de santé publique de la Montérégie (Guay); University of Victoria (Bramadat, Roy); University of British Columbia (Bettinger); Vaccine Evaluation Center, Women's Health Research Institute, and BC Women's and Children's Hospital (Bettinger); Representative for The Canadian Research Group on Religious and Cultural Reasons for Vaccine Hesitancy and Refusal (Dubé, Guay, Bramadat Roy, and Bettinger)
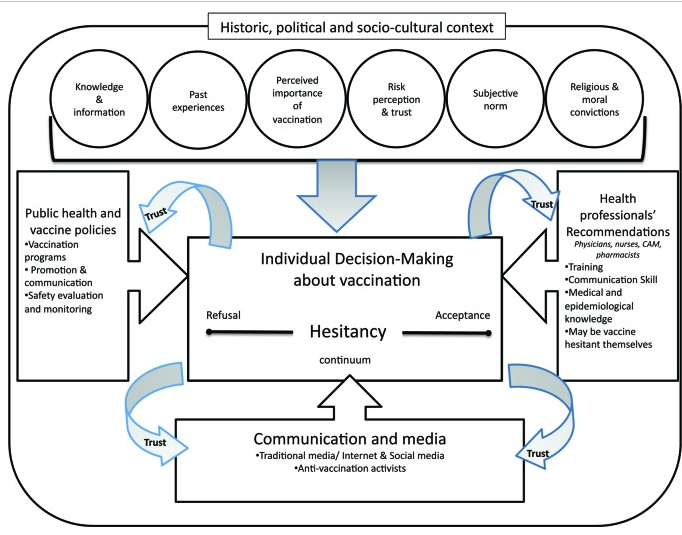
"[I]n addition to the factors affecting vaccine acceptance at the individual level, a thoughtful understanding of vaccine hesitancy needs to be grounded in the particular historical, political and socio-cultural context in which vaccination occurs. Consideration should also be given to broader influences on vaccine hesitancy such as the role of public health and vaccine policies, communication and media and health professionals."
This research review provides an overview of the phenomenon of vaccine hesitancy. It is premised on the observation that, while vaccination programmes have contributed to the decline in mortality and morbidity of various infectious diseases and are credited with the elimination of poliomyelitis in the Americas and the worldwide eradication of smallpox, to be successful in reducing the prevalence and incidence of vaccine-preventable diseases (VPD), vaccination programmes rely on a high uptake level.
Figure 1 on page 2 of the review presents a conceptual model consisting of 3 domains of factors that interact and could lead to vaccine hesitancy at the individual level. This model was adapted from a schema summary of discussions held during a workshop on the cultural and religious roots of vaccine hesitancy in which some 40 experts from various fields (social sciences, humanities, public health, biomedical sciences) met to share their views on vaccine hesitancy in the Canadian context. This model "illustrates that vaccine hesitancy is an individual behavior influenced by a range of factors, such as knowledge or past experiences. Vaccine hesitancy is also the result of broader influences and should always be looked at in the historical, political and socio-cultural context in which vaccination occurs. Trust placed in the system that delivers vaccines, in the health professionals who recommend and administer the vaccines, in the policy-makers who decide about vaccination programs and in the different types of information about vaccines conveyed in the media also mediates the impact of these factors on vaccine hesitancy."
Citing several studies examining determinants of vaccination decision-making to come to a definition of vaccine hesitancy, the authors find that the common ground among the models they explored is the fact that attitudes toward vaccination should be visualised on a continuum, ranging from active demand for vaccines to complete refusal of all vaccines. They note that, while a 15-item survey instrument developed in the United States (US) context to directly measure the level of vaccine hesitancy among parents "has shown promising results", such efforts are not new; the Health Belief Model was originally developed in the 1950s to look at barriers to polio vaccination among parents.
The review looks at research that describes the roles of the following arenas/personnel in vaccine hesitancy, such as:
- The historical, political, and socio-cultural context. For example: "The rise of the informed patient has shifted the traditional locus of power from doctors as sole directors of patient care to shared decision-making between health professionals and patients who want to be active participants in the decision-making process concerning their health."
- Media and communication. The authors note that "more research is needed to assess whether individuals who already have concerns regarding vaccination are more likely to search for information on the Internet from a range of sources or whether it is the Internet searches themselves that generate concerns regarding vaccination."
- Public health and vaccine policies. A key point from this section of the review: "Public health has a role to play in communicating adequately with the population. High quality vaccine safety surveillance is in place in developed countries. However, the strength and reliability of these systems is not well-understood by the population or even by some healthcare providers. Inaccurate information regarding both vaccine safety and the process leading to vaccine licensure and inclusion in universal programs circulates widely..."
- Health professionals. Amongst other articles cited in this section of the review, the authors point to several of them that articulate the importance of maintaining a trustworthy patient-provider relationship and the importance of tailoring the communication to specific patients' concerns and doubts.
- The individual decision-making process. "The overwhelming majority of studies looking at determinants of vaccine acceptance have been conducted among parents, mainly because most vaccines are targeted at children and adolescents. These reviews had different objectives and scopes, making it difficult to draw definitive conclusions regarding the most influential factors in vaccine acceptance or refusal."
- Knowledge/information about vaccination. Based on their review, the authors concluded that the association between level of knowledge about vaccination and vaccine acceptance is not straightforward.
- Past experiences with vaccination services. For example, "negative encounters with vaccine providers, can influence future decision-making regarding vaccination."
- Perceptions of the importance of vaccination in maintaining health. One study described here showed that "vaccines are seen as something that would perturb rather than boost the immune system. Indeed, studies conducted among parents consistently show that concerns regarding the number of vaccines and doses as well as the age at first vaccination are associated with delayed vaccination or vaccine refusal."
- Health professionals' recommendations and use of complementary and alternative medicine (CAM). One study cited here "quantifies a striking influence of homeopathy on the belief that vaccinations could harm the immune system."
- Risk perceptions. "Perceptions of risk can influence vaccine decision-making in two ways: perceived risks of VPD can foster vaccine acceptance and perceived risks of vaccines can contribute to vaccine refusal. This is further complicated by the fact that vaccines are administered as prophylactics to healthy individuals and the risks of vaccines (real or alleged) are visible while their benefits are impossible to evaluate from an individual perspective. In addition, the decision not to vaccinate is reversible, while the opposite is not true."
- Trust. The authors cite several studies, one of which cautions researchers not to use too narrow a concept of trust when studying vaccination acceptance and refusal. This particular study involved field work in Brighton, United Kingdom (UK), and several countries in West Africa, which led to the conclusion that "the concept of trust was rarely evoked by parents when describing their relationships with health professionals. More significant was whether parents felt supported and confident to ask questions and to express their views when discussing about vaccines with doctors or other health professionals."
- Subjective norm, social pressure, and social responsibility. "Seeing vaccination as a social norm is a potentially powerful driver of vaccine acceptance."
- Moral or religious convictions. "[V]accination refusal is sometimes linked with philosophical beliefs or moral convictions regarding health and immunity, such as a preference for “natural” over “artificial” medicines. Refusal of vaccines has also been linked with strong religious convictions. Orthodox Protestants in The Netherlands and the Amish in the United States are religious communities well-known for rejecting vaccination..."
In concluding the review, the authors state that "experts worldwide acknowledge that there is an increasing trend toward vaccine hesitancy." Many of these experts have proposed ways to counter vaccine hesitancy at the population level, including increasing transparency in policymaking decisions regarding vaccination programmes, providing education and information to the public and health providers about the process that leads to approval of new vaccines, and diversifying post-marketing surveillance of vaccine-related adverse events. They sum up their review by reiterating that "individual decision-making regarding vaccination is complex and involves emotional, cultural, social, spiritual and political factors as much as cognitive factors."
Human Vaccines & Immunotherapeutics 9:8, 1763-1773; August 2013; © 2013 Landes Bioscience. Sent from Michael Favin to The Communication Initiative on February 23 2015.
- Log in to post comments