











































Comparisons of Vaccine Hesitancy across Five Low- and Middle-Income Countries
University of Michigan (Wagner, Masters, Gebremeskel, Boulton); University of Colorado Anschutz Medical Campus (Domek, Asturias); Colorado School of Public Health (Domek, Asturias); Post Graduate Institute of Medical Education and Research (Mathew); Shanghai Municipal Centers for Disease Control & Prevention (Sun, Ren, Huang); Universidad del Valle de Guatemala (Contreras-Roldan); University of Michigan Medical School (Boulton)
"Continued surveillance of attitudes towards vaccination in LMICs can help identify shifts in future opinions on vaccination attitudes."
Vaccine uptake can be thought of as the result of the 5 As: access, affordability, awareness, activation (e.g., cues such as short message service (SMS) reminders), and acceptance. Vaccine hesitancy is a continuum of behaviours ranging from delay in receipt to vaccination refusal. Using previously conducted studies from 5 low- and middle-income countries (LMICs) - including published studies from Guatemala, Ethiopia, and China, along with unpublished data from India and Bangladesh - this study aims to describe and compare vaccine hesitancy in five LMICs.
Mothers of children in Sirajganj, Bangladesh (n = 60), Shanghai, China (n = 788), Addis Ababa, Ethiopia (n = 341), Guatemala City and Quetzaltenango, Guatemala (n = 767), and Chandigarh, India (n = 309) completed a survey between 2016 and 2018 using the World Health Organization (WHO) Strategic Advisory Group of Experts on Immunization (SAGE) Vaccine Hesitancy Scale's 10-item Vaccine Hesitancy Scale. The scores of different constructs were compared across countries and by the mother's education level using linear regression models with generalized estimating equations.
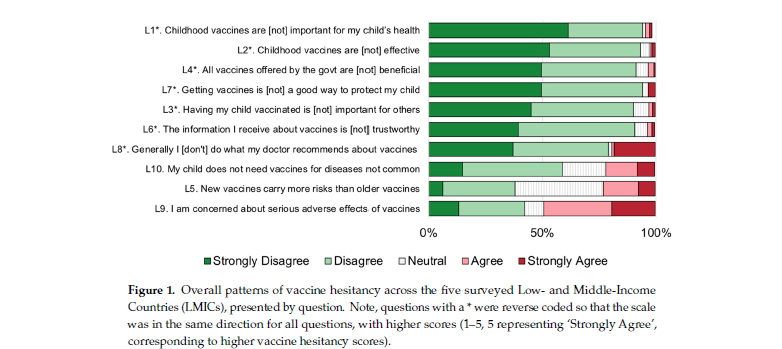
A large majority of surveyed participants agreed or strongly agreed that "childhood vaccines are important for my child's health" (95%), that "childhood vaccines are effective" (93%), and that "getting vaccines is a good way to protect my child" (94%). Around 90% of responders agreed or strongly agreed that "all vaccines offered by the government are beneficial", "having my child vaccinated is important for others", and "the information I receive about vaccines is trustworthy". However, fewer respondents agreed that they follow their doctor's recommendations about vaccines (79%).
Compared to mothers in China, mothers in Bangladesh perceived less vaccination benefit; however, mothers in Ethiopia and Guatemala perceived greater benefit. Compared to Chinese mothers, mothers in Bangladesh, India, Guatemala, and Ethiopia thought new vaccines less risky and, in 3 of these countries, had less concern about side effects (India, Bangladesh, and Ethiopia). Belief that some vaccines are no longer needed was less common in Ethiopia and Guatemala, and more common in Bangladesh (though not significant) and India compared to China.
In reflecting on the findings, the researchers note that the differences they saw between sites could be due to background education levels in the population (though education level was not significantly linked with vaccine hesitancy), exposure to different social and traditional media, and trust in the government, for example. Medical and political populism has also been linked to changes in vaccination attitudes.
Thus, they suggest that local circumstances are important to consider when developing programmes to promote vaccines and call for more research to understand socio-cultural influences on vaccine decision-making. For instance, studies in high-income countries have found consistent associations about education and vaccine hesitancy, which were not part of the findings here.
In conclusion, while there are no easy solutions to alleviating vaccine hesitancy, in light of the fact that "doctors are seen as important sources of health information throughout the world, it will be key to give doctors the tools and education needed to deal with vaccine hesitancy, for instance, through nudges or talking about experiences with patients who had vaccine-preventable diseases..."
Vaccines 2019, 7(4), 155; https://doi.org/10.3390/vaccines7040155.
- Log in to post comments