











































System within Systems: Challenges and Opportunities for the Expanded Programme on Immunisation in Pakistan
Health Services Academy (Haq, Shaikh, Hafeez); Alliance for Health Policy & Systems Research (Tran, Ghaffar)
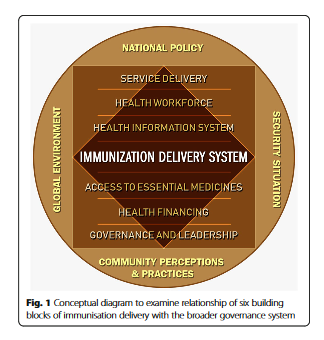
"Exploring the views of immunisation programme staff in the context of...building blocks interacting with each other, and with the larger ecology, can help us understand the barriers as well as facilitators to the programme implementation."
With only two-thirds of children receiving full immunisation, Pakistan is among those countries where immunisation rates have been chronically low. The country started its Expanded Programme on Immunisation (EPI) in 1978, and a high-level Emergency Operations Centre (EOC) was established after polio was declared a national emergency in 2014. In that context, this study explores the views of policymakers, managers, and staff working at different levels in an effort to understand the building blocks of Pakistan's immunisation delivery system and their relationship with those of the wider health system, to examine how the factors from the outer social ecology impact this service delivery, and to document the challenges and opportunities that arise from these complex relationships.
The study uses the World Health Organization (WHO)'s concept of 6 building blocks, which include service delivery, health workforce, health information system, access to essential medicines, financing, and governance and leadership. Some have critiqued this framework, suggesting that it oversimplifies phenomena that are complex and have a dynamic relationship with each other and with the world outside of this system. Thus, the researchers of the present study propose that the EPI programme of Pakistan, with its own set of 6 building blocks, operates within the building blocks of the larger health system, both having a continuous interaction with each other. Moreover, these two also have a dynamic interface with the outer ecology, which includes factors such as community perceptions and vaccine hesitancy.
The researchers carried out a qualitative case study comprised of semi-structured, in-depth interviews with 34 purposively selected key informants from various tiers of immunisation policy and programme implementation. The interviews revealed that the EPI faces several challenges, including those related to:
- Service delivery: There is a lack of clarity on whether to provide vaccination through fixed centres or mobile teams. This debate emerged from years of door-to-door campaigns for polio, which was decided by the broader governance and has raised public expectations. In addition, EPI is reportedly unable to plan for and provide services to the mobile, marginalised, and hard-to-reach populations. A closely connected point, which is also a solution, is the issue of population estimates; there is presently a lack of accurate population data.
- Health workforce: Participants pointed to a scarcity of human resource and capacity at various levels; additional vaccinators, especially females, are required. Coupled with this is a dearth of succession planning and recurrent transfers within management tiers, which leads to a loss of institutional memory and limited levels of knowledge transfer.
- Health information system: Almost all participants mentioned room for improvement in the data credibility and accountability. The current lack of accurate information about the number of children to be reached leads to inaccurate planning, false reporting, and pilferage of resources. One interviewee said, "There is no single and comprehensive source of family data that vaccinator can use to plan their demand and ultimate delivery of the vaccine. Micro-census in both urban and rural areas is the solution to ascertain the correct denominator of children to be vaccinated."
- Essential medicines (vaccines and supplies): For example, some highlighted the importance of accurate recording and reporting of vaccine availability, its storage, utilisation, and wastage, citing a few examples where vaccines were apparently being consumed but not actually administered.
- Health financing: There appears to be a lack of a separate budget line for EPI.
- Governance and leadership: Coordination issues seemed particularly important to participants when they explained governance challenges that emerge from the implementation of RI and polio eradication through two separate arms of the same programme. Participants stressed the need to define the role of the national ministry and strengthen mechanisms for inter-provincial coordination.
- Global environment: Two factors - global interest in polio eradication and the war on terror - were most commonly mentioned. For instance, one interviewee said, "Polio started receiving much more funding, visibility and authority, ignoring sometimes the fact that it was a strong RI [routine immunisation] that would ultimately guarantee the sustainable eradication of polio."
- National policy: Health policy has always had a focus on "sickness care" rather than preventing disease and promoting health in the country. The question of how to enhance coverage through the involvement of the private sector, which currently contributes only 3% of the total immunisation, was also discussed.
- Security situation: The participants explained how, in the wake of 9/11, the global war on terror and the geopolitical situation of Pakistan and Afghanistan impacted polio eradication and other immunisation efforts in the country - e.g., necessitating an additional layer of security for immunisation workers.
- Community perceptions and practices: Almost all interviewees talked about demand-side issues and highlighted the need to address community misperceptions and facilitate immunisation behaviours. They suggested that it is mainly the conservative minded, blind followers of faith leaders, or nomads who usually refuse RI. One participant from the federal EPI explained that "A common feature is that these people do not usually have enough knowledge of the purpose and benefits of vaccines; providing this information usually proves helpful. The challenge is that misperceptions may not be the same across provinces and districts; hence a blanket communication is less likely to work. Exploring the local factors and perceptions that may be acting as a barrier and integrating this with other public health communication is required." Participants also commented that the local and mass media components of the current communication campaigns do not complement each other, because of which the quantum of effect is lost. In the words of one participant, "Local campaigns should address the local misperceptions while also establishing a connection with the mass media messages, which are there to sensitise the masses on importance of immunisation while reinforcing the content being disseminated at the local level, at the same time."
The researchers observe that many of the gaps arise at points where EPI has an interaction with the broader health and governance; thus, their improvement also requires concerted efforts of the entire system. That is, certain decisions, such as providing policy on dealing with an unregulated private sector, negotiating local and global security, and setting local and national priorities in the wake of a global push for just one disease (i.e., polio), are the responsibility of the broader governance system. Their assertion is that "immunisation in Pakistan could be improved if EPI were to be fully integrated within the broader health system."
In conclusion: "The synergised engagement of local, national and global stakeholders can go a long way in improving the country's immunisation system, global health security, and achievement of the sustainable development goals."
Health Research Policy and Systems (2019) 17:51 https://doi.org/10.1186/s12961-019-0452-z
- Log in to post comments