











































Vaccination Uptake and Income Inequalities within a Mass Vaccination Campaign
The Max Stern Yezreel Valley College (Tur-Sinai); Ben-Gurion University of the Negev (Gur-Arie, Davidovitch, Glazer); Tel Aviv University (Kopel); Israel Ministry of Health (Glazer, Anis, Grotto)
"How health inequalities influence economic, social, cultural and political aspects of public heatlh continues to plague researchers, policymakers, and decision makers..."
Populations of low socioeconomic status (SES) oftentimes have not only economic but also social barriers to overcome in order to receive healthcare services. Health disparities/inequalities generally affect disadvantaged social groups disproportionately. This study analyses the vaccination uptake rates resulting from a mass polio vaccination campaign carried out in Israel in July 2013 on the basis of health inequality parameters of SES, principles of solidarity, and the Gini inequality index, which is designed to reveal unexpected contributors to health inequalities, such as illiteracy, in different societies.
Given Israel's collective memory of the 1950s polio epidemic, Ministry of Health (MoH) officials were concerned with the potential of another outbreak following isolation of wild polio virus 1 (WPV1) in sewage in 2013. The presence of WPV1 in sewage-sampling sites in central Israel was detected mostly around Arab or mixed Jewish-Arab communities, whereas there were only 3 positive sewage samples in the West Bank and one in the Gaza Strip. The MoH opted to take national preventive action by administering oral poliovirus vaccine (OPV) to all children born after January 1 2004 who had received at least one dose of inactivated poliovirus vaccine (IPV) in the past. During the campaign, the need for collective action that would not directly benefit the individual became apparent. In communications, concepts of "society" and "solidarity" were used in different ways by different actors to persuade and evoke compliance.
The study is based on data gathered from the MoH's administrative records from mother-and-child clinics across Israel. The research population is comprised of resident infants and children whom the MoH defined as eligible for the OPV between August and December 2013 (the "campaign period"). The analysis was carried out as follows: The first goal of the study - profiling Israel's 2013 polio vaccination programme - was complemented by various descriptive statistical indicators. The second goal - determining the correlation between vaccination uptake among varied social groups as measured on the basis of social and economic indicators - was attained by the use of: (i) the SES index (for statistical areas and municipalities), which indicates the socio-demographic, social, and economic characteristics of the populations served; and (ii) the Gini inequality index (for municipalities), whereby the closer the Gini is to 0, the smaller the health inequalities are; as the Gini gets closer to 1, inequalities are greater.
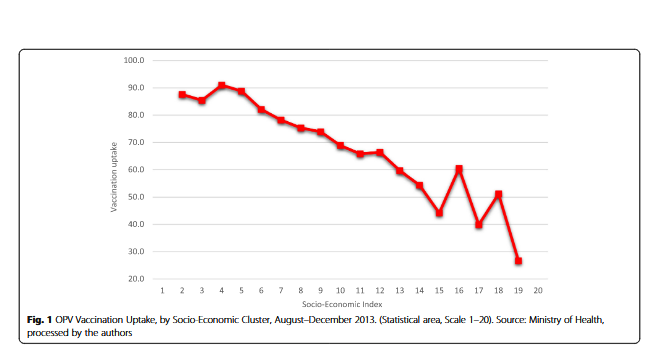
The central finding of the study is that the higher the SES level of the municipality where the mother-and-child clinic is located, the lower the OPV vaccination uptake is. The greater the income inequality is (Gini index) in the municipality where the mother-and-child clinic is situated, the lower the vaccination uptake. Put another way: "This study shows that in communities that are stronger socio-economically, there is less inclination for parents to ensure that their children are vaccinated. Additionally, in municipalities where there are smaller economic gaps and community members are more similar in SES status, there is a greater tendency to vaccinate their children against polio."
The analysis also revealed that the average vaccination uptake among municipalities in low-SES and low income-inequality levels was nearly 90% at the end of the campaign period. Among municipalities in low-SES areas typified by high income inequality indices, vaccination uptake was nearly 80%. Average vaccination uptake in municipalities in high-SES areas, at the end of the campaign period, was 50% in municipalities with low income inequality and roughly 40% in municipalities with high income inequality. Per the researchers: "The overall success of the campaign may be partly attributed to the Israeli focus on safety of the family and solidarity for others as motives for vaccination...Nevertheless, the variance in vaccine uptake rates shows that Israel has differing vaccination uptake among different SES clusters of society."
In other words, the researchers observe that "Compliance with or opposition to vaccination falls within the limits of state power in the private sphere (like family, religion, and health beliefs) that is often emphasized by ethnic tensions....Thus, Israel's 2013 polio vaccination campaign is intricately linked to, and must be understood in the context of communities' social standing..." In that light, they call on public health professionals promoting vaccine programmes to understand the decision to vaccinate in larger social contexts, in contrast to viewing vaccination as an individualised decision alone. This recommendation is not unique to Israel, they stress: "Policymakers are encouraged to strengthen principles of solidarity in their efforts to eradicate SES and equality disparities in healthcare..."
The researchers urge future research on the correlation between the solidarity and the Gini inequality index (for example, in terms of health behaviour) in order to contextualise and apply this study's findings. "The results of this study promote further investigations into the correlation between solidarity and different aspects of society and culture. In the meantime, stakeholders and decision-makers are urged to incorporate SES and solidarity into vaccination policy and health policy in general."
In conclusion, the researchers hope the study provides insights into how vaccination campaigns should be organised in order to maximise vaccination uptake, taking into account the unique circumstances of particular localities. More specifically, "Public health professionals promoting vaccine programs need to make specially-designed efforts both in localities with high average income and in localities with a high level of income diversity/inequality." These efforts may very well rest on the conviction that: "Solidarity helps to close health disparities."
Israel Journal of Health Policy Research. 2019; 8: 63. doi: 10.1186/s13584-019-0324-6.
- Log in to post comments