











































Increasing Vaccine Uptake in Low- and Middle-Income Countries: Opportunities for Behavioural Insights Research
The Behavioural Insights Team
There is increasing awareness in the global health community that barriers to vaccine uptake include not only structural factors but those related to individual behaviour and decision-making as well. Underpinned by a "dual-process" model that recognises the biases inherent in the way we behave and make decisions, "behavioural insights" uses evidence of the conscious and non-conscious drivers of human behaviour to address practical issues. Drawing on this approach, and with support from the Wellcome Trust, the Behavioural Insights Team produced a landscape analysis of opportunities for behavioural insights research to increase vaccine uptake in low- and middle-income countries (LMICs). This report details the findings from that review.
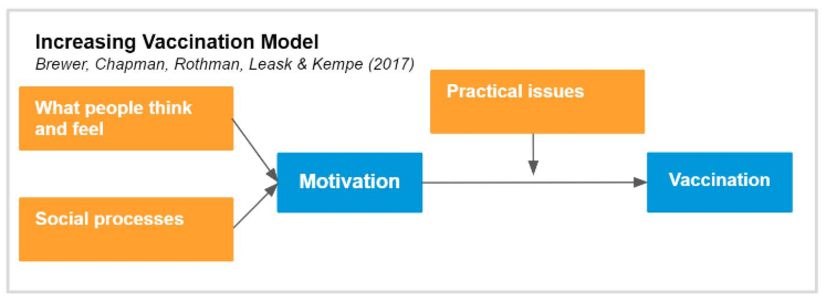
Part A sets out a review of existing evidence from behavioural insights research on vaccine uptake. It begins with the assertion that several of the attributes of vaccination make people vulnerable to bias in making vaccination decisions. Namely, the outcomes of vaccination are uncertain (for example, people aren't sure they will contract the disease if they are not immunised, but vaccination might cause side effects), and the benefits and costs of vaccination occur at different points in time and may accrue to people other than the decision maker (particularly in the case of childhood vaccination). Brewer et al. have proposed the Increasing Vaccination Model, above, to help structure thinking about the behavioural barriers to vaccination. The model suggests that people's attitudes and wider social processes jointly influence people's motivations and intentions towards vaccination. Practical barriers then mediate the relationship between favourable intentions to vaccinate and ultimate vaccination behaviour. In other words, we shouldn't assume that because an intervention changed attitudes and intentions towards vaccination that it will translate into behaviour change (the "intention-behaviour gap" in vaccination behaviour).
Section 1 describes in detail the existing evidence from LMIC settings, most of which focuses on encouraging vaccine demand (i.e., both promoting favourable intentions towards vaccination among potential recipients and breaking down practical barriers that might prevent or discourage people from receiving vaccinations). The researchers identified 28 studies published since 2010 evaluating the effect of behavioural interventions intended to increase demand for vaccinations in LMIC settings. The evidence in this area was generally assessed to be low or very low quality according to the widely used GRADE framework. In sum:
Education and information about vaccines:
- There is some evidence that centre-based education, in-home education with visual aids, and redesigned immunisation cards are effective in increasing childhood vaccination uptake in Asia.
- There is no evidence that loss- or gain-frame messaging is more effective in encouraging vaccine uptake in LMIC settings, but this was only tested in one study.
- There is insufficient evidence about planning and implementation intentions to draw any conclusion about the effectiveness of these strategies in a LMIC context.
Incentives for vaccination:
- The limited available evidence is inconclusive as to whether cash transfer programmes are effective at increasing vaccine uptake in LMIC settings.
- There is some evidence that small, compliance-linked incentives increase infant vaccine uptake.
- One study found that a pay-for-performance scheme for primary healthcare providers was no more effective in encouraging vaccine uptake than traditional input-based financing.
Reminders and recalls for vaccination appointments:
- Reminder and recall messages sent to mobile phones are generally effective at encouraging infant vaccine uptake and on-time infant vaccine uptake.
- No studies were found that varied reminder message content to investigate which messages are most effective at encouraging parents to bring their children to vaccination appointments.
- Reminder and recall messages are an effective component of systems to track vaccine doses within the population.
Use of social networks to encourage vaccination:
- Using social signaling to highlight social norms in favour of vaccination is promising, but there has only been one high-quality trial in this area.
- One study found vaccination discussion groups with influential members of the community in Pakistan increased childhood vaccine uptake.
The landscape review did not identify any standalone interventions focused on changing individual behaviour to improve the supply of vaccines and vaccine services in LMICs. However, 3 studies evaluated vaccine stock-tracking technology systems that drew on behavioural techniques, finding that the new technology increased vaccine availability or quality of vaccine tracking data. However, these interventions were generally less rigorously evaluated than the demand-side interventions described above.
Section 2 summarises the outputs of comparable research conducted in high-income countries (HICs). In sum:
Changing what people think and feel about vaccination:
- Substantial evidence suggests that neither loss- or gain-framed messages are more effective in encouraging vaccination behaviour.
- Most studies that have successfully changed the way people perceive the risks of vaccine-preventable diseases have not demonstrated any subsequent impact on vaccination behaviour.
- Evidence suggests that educational interventions to increase childhood vaccine uptake are more effective in LMICs than in HICs. In general, educational interventions have not been effective at increasing vaccine uptake in HICs.
- There is some evidence to suggest that motivational interviewing has a moderate positive impact on vaccine uptake.
Using social processes to encourage vaccination:
- Correlational studies suggest that interventions that highlight social norms in favour of vaccination could increase vaccine uptake, but no studies were found that tested such interventions.
- Available evidence suggests that providing performance feedback to primary healthcare providers has a modest positive effect on vaccine uptake.
- Limited evidence suggests that emphasising the pro-social nature of vaccination behaviour has little if any impact on vaccine uptake.
- There is considerable evidence that healthcare provider recommendations increase vaccine uptake.
Bridging the gap between motivation and behaviour:
- Available evidence suggests that interventions that set vaccination as the default, such as automatic appointment scheduling, presumptive announcements, and vaccine requirements, are effective at increasing vaccine uptake.
- Limited evidence indicates that requiring people to make an active choice about vaccination is moderately effective at increasing uptake.
- There is good evidence that reducing friction costs increases uptake of vaccinations.
- Timely interventions that prompt people to plan when they will get vaccinated or remind them of upcoming appointments increase vaccination.
- Strong evidence suggests that incentives, structured as either rewards or sanctions, are effective at encouraging vaccination.
Part B of this report sets out future opportunities for behavioural insights research to encourage vaccine uptake in LMICs in light of the evidence gaps identified in Part A. The recommendations are structured around a 4-part framework that categorises options for funding research in this area. First, in light of the fact that behavioural barriers and solutions are to some extent context specific, 'Focus' provides an initial lens for deciding which undervaccinated populations to focus on, with the objective of maximising impact. Following on from the 'Focus' stage are 3 broad approaches to behavioural insights research on encouraging vaccine uptake in LMICs. The decision of which approach is most appropriate for a given context should be informed by the barriers to vaccination in the intended population, the state of existing evidence for encouraging vaccine uptake in that population, and whether behavioural insights is the central component of the intervention approach:
- Refine: Develop behaviourally informed solutions where there is existing evidence of effectiveness in encouraging vaccine uptake. This would involve testing different variants of interventions in similar contexts, or testing interventions (based on those) that have worked in HICs, in LMIC settings.
- Expand: Fund research into behaviourally informed solutions that haven't yet been applied to vaccination behaviour in LMIC settings. Solutions based on encouraging results from correlational research could be developed and tested.
- Enhance: Capitalise on the role behavioural insights could play in maximising impact and effectiveness where behaviourally informed interventions are not the central component of a given solution. Options under this approach include applying behavioural insights to improve the effectiveness of new technology, support evidence dissemination, or scale up impactful solutions.
Specific suggestions for funders in light of this analysis are offered. For example, they "could invest in creating and facilitating networks to enable sharing of evidence and best-practice in the vaccine community. Remembering the importance of trusted messengers in encouraging behaviour change, it would be valuable for such networks to include researchers from LMICs, country-decision makers and managers of vaccination programmes. Participants can learn about best-practice but also attend as co-creators and advocates of successful interventions."
In conclusion: "It would be valuable to meet with representatives of national immunisation technical advisory groups(NITAGs), implementing organisations and the WHO to better understand the barriers to implementing evidence-based practice to encourage vaccination. Are these organisations limited by a paucity of cost-effective solutions to encourage vaccine uptake, or is it that the available evidence does not reach the right people in an interpretable and actionable format? Answers to these questions can inform the direction of research in this area."
BI Team website, April 29 2020.
- Log in to post comments